
mycophenolic acid
These highlights do not include all the information needed to use MYCOPHENOLIC ACID DELAYED-RELEASE TABLETS safely and effectively. See full prescribing information for MYCOPHENOLIC ACID DELAYED-RELEASE TABLETS. MYCOPHENOLIC ACID delayed-release tablets, for oral use Initial U.S. Approval: 2004
bc38bc5e-7f0a-4419-81ec-04726ce47421
HUMAN PRESCRIPTION DRUG LABEL
Feb 13, 2023
PD-Rx Pharmaceuticals, Inc.
DUNS: 156893695
Products 2
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
mycophenolic acid
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (14)
mycophenolic acid
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (16)
Drug Labeling Information
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
1.1 Prophylaxis of Organ Rejection in Kidney Transplant
Mycophenolic acid delayed-release tablets are indicated for the prophylaxis of organ rejection in adult patients receiving a kidney transplant.
Mycophenolic acid delayed-release tablets are indicated for the prophylaxis of organ rejection in pediatric patients 5 years of age and older who are at least 6 months post kidney transplant.
Mycophenolic acid delayed-release tablets are to be used in combination with cyclosporine and corticosteroids.
1.2 Limitations of Use
Mycophenolic acid delayed-release tablets and mycophenolate mofetil (MMF) tablets and capsules should not be used interchangeably without physician supervision because the rate of absorption following the administration of these two products is not equivalent.
- Mycophenolic acid delayed-release tablets are an antimetabolite immunosuppressant indicated for prophylaxis of organ rejection in adult patients receiving kidney transplants and in pediatric patients at least 5 years of age and older who are at least 6 months post kidney transplant. ( 1.1)
- Use in combination with cyclosporine and corticosteroids. ( 1.1)
Limitations of Use:
- Mycophenolic acid delayed release tablets and mycophenolate mofetil tablets and capsules should not be used interchangeably. ( 1.2)
WARNINGS AND PRECAUTIONS SECTION
5 WARNINGS AND PRECAUTIONS
5.1 Embryo-Fetal Toxicity
Use of mycophenolic acid delayed-release tablets during pregnancy is associated with an increased risk of first trimester pregnancy loss and an increased risk of congenital malformations, especially external ear and other facial abnormalities, including cleft lip and palate, and anomalies of the distal limbs, heart, esophagus, kidney, and nervous system. Females of reproductive potential must be aware of these risks and must be counseled regarding pregnancy prevention and planning. Avoid use of mycophenolic acid delayed-release tablets during pregnancy if safer treatment options are available [see Use in Specific Populations (8.1, 8.3)].
5.2 Management of Immunosuppression
Only physicians experienced in immunosuppressive therapy and management of organ transplant patients should prescribe mycophenolic acid delayed-release tablets. Patients receiving the drug should be managed in facilities equipped and staffed with adequate laboratory and supportive medical resources. The physicians responsible for maintenance therapy should have complete information requisite for the follow-up of the patient [ see Boxed Warning].
5.3 Lymphoma and Other Malignancies
Patients receiving immunosuppressants, including mycophenolic acid delayed- release tablets, are at increased risk of developing lymphomas and other malignancies, particularly of the skin [ see Adverse Reactions (6)]. The risk appears to be related to the intensity and duration of immunosuppression rather than to the use of any specific agent.
As usual for patients with increased risk for skin cancer, exposure to sunlight and UV light should be limited by wearing protective clothing and using a broad-spectrum sunscreen with a high protection factor.
Post-transplant lymphoproliferative disorder (PTLD) has been reported in immunosuppressed organ transplant recipients. The majority of PTLD events appear related to Epstein-Barr Virus (EBV) infection. The risk of PTLD appears greatest in those individuals who are EBV seronegative, a population which includes many young children.
5.4 Serious Infections
Patients receiving immunosuppressants, including mycophenolic acid delayed- release tablets, are at increased risk of developing bacterial, viral, fungal, and protozoal infections, and new or reactivated viral infections, including opportunistic infections [ see Warnings and Precautions (5.5)]. These infections may lead to serious, including fatal outcomes. Because of the danger of oversuppression of the immune system which can increase susceptibility to infection, combination immunosuppressant therapy should be used with caution.
5.5 New or Reactivated Viral Infections
Polyomavirus associated nephropathy (PVAN), JC virus-associated progressive multifocal leukoencephalopathy (PML), cytomegalovirus (CMV) infections, reactivation of hepatitis B (HBV) or hepatitis C (HCV), SARS-CoV-2 infection, have been reported in patients treated with immunosuppressants, including MPA derivatives mycophenolic acid delayed-release tablets and MMF. Reduction in immunosuppression should be considered for patients who develop evidence of new or reactivated viral infections. Physicians should also consider the risk that reduced immunosuppression represents to the functioning allograft.
PVAN, especially due to BK virus infection, is associated with serious outcomes, including deteriorating renal function and renal graft loss. Patient monitoring may help detect patients at risk for PVAN.
PML, which is sometimes fatal, commonly presents with hemiparesis, apathy, confusion, cognitive deficiencies, and ataxia. Risk factors for PML include treatment with immunosuppressant therapies and impairment of immune function. In immunosuppressed patients, physicians should consider PML in the differential diagnosis in patients reporting neurological symptoms and consultation with a neurologist should be considered as clinically indicated.
The risk of CMV viremia and CMV disease is highest among transplant recipients seronegative for CMV at time of transplant who receive a graft from a CMV seropositive donor. Therapeutic approaches to limiting CMV disease exist and should be routinely provided. Patient monitoring may help detect patients at risk for CMV disease [ see Adverse Reactions (6.1)].
Viral reactivation has been reported in patients infected with HBV or HCV. Monitoring infected patients for clinical and laboratory signs of active HBV or HCV infection is recommended.
5.6 Blood Dyscrasias, Including Pure Red Cell Aplasia
Cases of pure red cell aplasia (PRCA) have been reported in patients treated with MPA derivatives in combination with other immunosuppressive agents. The mechanism for MPA derivatives induced PRCA is unknown; the relative contribution of other immunosuppressants and their combinations in an immunosuppressive regimen is also unknown. In some cases, PRCA was found to be reversible with dose reduction or cessation of therapy with MPA derivatives. In transplant patients, however, reduced immunosuppression may place the graft at risk. Changes to mycophenolic acid delayed-release tablets therapy should only be undertaken under appropriate supervision in transplant recipients in order to minimize the risk of graft rejection.
Patients receiving mycophenolic acid delayed-release tablets should be monitored for blood dyscrasias (e.g., neutropenia or anemia). The development of neutropenia may be related to mycophenolic acid delayed-release tablets itself, concomitant medications, viral infections, or some combination of these reactions. Complete blood count should be performed weekly during the first month, twice monthly for the second and the third month of treatment, then monthly through the first year. If blood dyscrasias occur [neutropenia develops (ANC < 1.3 × 10 3/mcL) or anemia], dosing with mycophenolic acid delayed-release tablets should be interrupted or the dose reduced, appropriate tests performed, and the patient managed accordingly.
5.7 Serious GI Tract Complications
Gastrointestinal bleeding (requiring hospitalization), intestinal perforations, gastric ulcers, and duodenal ulcers have been reported in patients treated with mycophenolic acid delayed-release tablets. Mycophenolic acid delayed-release tablets should be administered with caution in patients with active serious digestive system disease.
5.8 Acute Inflammatory Syndrome Associated with Mycophenolate Products
Acute inflammatory syndrome (AIS) has been reported with the use of mycophenolate products, and some cases have resulted in hospitalization. AIS is a paradoxical pro-inflammatory reaction characterized by fever, arthralgias, arthritis, muscle pain and elevated inflammatory markers including, C-reactive protein and erythrocyte sedimentation rate, without evidence of infection or underlying disease recurrence. Symptoms occur within weeks to months of initiation of treatment or a dose increase. After discontinuation, improvement of symptoms and inflammatory markers are usually observed within 24 to 48 hours. Monitor patients for symptoms and laboratory parameters of AIS when starting treatment with mycophenolate products or when increasing the dosage. Discontinue treatment and consider other treatment alternatives based on the risk and benefit for the patient.
5.9 Immunizations
During treatment with mycophenolic acid delayed-release tablets, the use of live attenuated vaccines should be avoided and patients should be advised that vaccinations may be less effective. Advise patients to discuss with the physician before seeking any immunizations
5.10 Rare Hereditary Deficiencies
Mycophenolic acid delayed-release tablets are inosine monophosphate dehydrogenase inhibitor (IMPDH inhibitor). Mycophenolic acid delayed-release tablets should be avoided in patients with rare hereditary deficiency of hypoxanthine-guanine phosphoribosyl-transferase (HGPRT), such as Lesch-Nyhan and Kelley-Seegmiller syndromes because it may cause an exacerbation of disease symptoms characterized by the overproduction and accumulation of uric acid leading to symptoms associated with gout, such as acute arthritis, tophi, nephrolithiasis or urolithiasis, and renal disease, including renal failure.
5.11 Blood Donation
Patients should not donate blood during therapy and for at least 6 weeks following discontinuation of mycophenolic acid delayed-release tablets because their blood or blood products might be administered to a female of reproductive potential or a pregnant woman.
5.12 Semen Donation
Based on animal data, men should not donate semen during therapy and for 90 days following discontinuation of mycophenolic acid delayed-release tablets [see Use in Specific Populations (8.3)].
- New or Reactivated Viral Infections: Consider reducing immunosuppression. ( 5.5)
- Blood Dyscrasias, including Pure Red Cell Aplasia (PRCA): Monitor for neutropenia or anemia; consider treatment interruption or dose reduction. ( 5.6)
- Serious GI Tract Complications (gastrointestinal bleeding, perforations and ulcers): Administer with caution to patients with active digestive system disease. ( 5.7)
- Immunizations: Avoid live attenuated vaccines. ( 5.9)
- Patients with Hereditary Deficiency of Hypoxanthine-guanine Phosphoribosyl-transferase (HGPRT): May cause exacerbation of disease symptoms; avoid use. ( 5.10)
- Blood Donation: Avoid during therapy and for 6 weeks thereafter. ( 5.11)
- Semen Donation: Avoid during therapy and for 90 days thereafter. ( 5.12)
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
7.1 Antacids With Magnesium and Aluminum Hydroxides
Concomitant use of mycophenolic acid delayed-release tablets and antacids decreased plasma concentrations of mycophenolic acid (MPA). It is recommended that mycophenolic acid delayed-release tablets and antacids not be administered simultaneously [ see Clinical Pharmacology (12.3)].
7.2 Azathioprine
Given that azathioprine and MMF inhibit purine metabolism, it is recommended that mycophenolic acid delayed-release tablets not be administered concomitantly with azathioprine or MMF.
7.3 Cholestyramine, Bile Acid Sequestrates, Oral Activated Charcoal and
Other Drugs That Interfere With Enterohepatic Recirculation
Drugs that interrupt enterohepatic recirculation may decrease MPA plasma concentrations when coadministered with MMF. Therefore, do not administer mycophenolic acid delayed-release tablets with cholestyramine or other agents that may interfere with enterohepatic recirculation or drugs that may bind bile acids, e.g., bile acid sequestrates or oral activated charcoal, because of the potential to reduce the efficacy of mycophenolic acid delayed-release tablets [ see Clinical Pharmacology (12.3)].
7.4 Sevelamer
Concomitant administration of sevelamer and MMF may decrease MPA plasma concentrations. Sevelamer and other calcium-free phosphate binders should not be administered simultaneously with mycophenolic acid delayed-release tablets [ see Clinical Pharmacology (12.3)].
7.5 Cyclosporine
Cyclosporine inhibits the enterohepatic recirculation of MPA, and therefore, MPA plasma concentrations may be decreased when mycophenolic acid delayed- release tablets are coadministered with cyclosporine. Clinicians should be aware that there is also a potential change of MPA plasma concentrations after switching from cyclosporine to other immunosuppressive drugs or from other immunosuppressive drugs to cyclosporine in patients concomitantly receiving mycophenolic acid delayed-release tablets [ see Clinical Pharmacology (12.3)].
7.6 Norfloxacin and Metronidazole
MPA plasma concentrations may be decreased when MMF is administrated with norfloxacin and metronidazole. Therefore, mycophenolic acid delayed-release tablets are not recommended to be given with the combination of norfloxacin and metronidazole. Although there will be no effect on MPA plasma concentrations when mycophenolic acid delayed-release tablets are concomitantly administered with norfloxacin or metronidazole when given separately [ see Clinical Pharmacology (12.3)].
7.7 Rifampin
The concomitant administration of MMF and rifampin may decrease MPA plasma concentrations. Therefore, mycophenolic acid delayed-release tablets are not recommended to be given with rifampin concomitantly unless the benefit outweighs the risk [ see Clinical Pharmacology (12.3)].
7.8 Hormonal Contraceptives
In a drug interaction study, mean levonorgestrel AUC was decreased by 15% when coadministered with MMF. Although mycophenolic acid delayed-release tablets may not have any influence on the ovulation-suppressing action of oral contraceptives, additional barrier contraceptive methods must be used when mycophenolic acid delayed-release tablets are coadministered with hormonal contraceptives (e.g., birth control pill, transdermal patch, vaginal ring, injection, and implant) [see Warnings and Precautions (5.1), Use in Specific Populations (8.3), Clinical Pharmacology (12.3)].
7.9 Acyclovir (Valacyclovir), Ganciclovir (Valganciclovir), and Other Drugs
That Undergo Renal Tubular Secretion
The coadministration of MMF and acyclovir or ganciclovir may increase plasma concentrations of mycophenolic acid glucuronide (MPAG) and acyclovir/valacyclovir/ganciclovir/valganciclovir as their coexistence competes for tubular secretion. Both acyclovir/valacyclovir/ganciclovir/valganciclovir and MPAG concentrations will be also increased in the presence of renal impairment.
Acyclovir/valacyclovir/ganciclovir/ valganciclovir may be taken with mycophenolic acid delayed-release tablets; however, during the period of treatment, physicians should monitor blood cell counts [ see Clinical Pharmacology (12.3)].
7.10 Ciprofloxacin, Amoxicillin Plus Clavulanic Acid and Other Drugs That
Alter the Gastrointestinal Flora
Drugs that alter the gastrointestinal flora, such as ciprofloxacin or amoxicillin plus clavulanic acid may interact with MMF by disrupting enterohepatic recirculation. Interference of MPAG hydrolysis may lead to less MPA available for absorption when mycophenolic acid delayed-release tablets are concomitantly administered with ciprofloxacin or amoxicillin plus clavulanic acid. The clinical relevance of this interaction is unclear; however, no dose adjustment of mycophenolic acid delayed-release tabletsis needed when coadministered with these drugs [ see Clinical Pharmacology (12.3)].
7.11 Pantoprazole
Administration of pantoprazole at a dose of 40 mg twice daily for 4 days to healthy volunteers did not alter the pharmacokinetics of a single dose of mycophenolic acid delayed-release tablets [ see Clinical Pharmacology (12.3)].
- Antacids with Magnesium and Aluminum Hydroxides: Decreases concentrations of MPA; concomitant use is not recommended. ( 7.1)
- Azathioprine: Competition for purine metabolism; concomitant administration is not recommended. ( 7.2)
- Cholestyramine, Bile Acid Sequestrates, Oral Activated Charcoal, and Other Drugs that Interfere with Enterohepatic Recirculation: May decrease MPA concentrations; concomitant use is not recommended. ( 7.3)
- Sevelamer: May decrease MPA concentrations; concomitant use is not recommended. ( 7.4)
- Cyclosporine: May decrease MPA concentrations; exercise caution when switching from cyclosporine to other drugs or from other drugs to cyclosporine. ( 7.5)
- Norfloxacin and Metronidazole: May decrease MPA concentrations; concomitant use with both drugs is not recommended. ( 7.6)
- Rifampin: May decrease MPA concentrations; concomitant use is not recommended unless the benefit outweighs the risk. ( 7.7)
- Hormonal Contraceptives: May reduce the effectiveness of oral contraceptives. Additional barrier contraceptive methods must be used. ( 5.2, 7.8)
- Acyclovir, Valacyclovir, Ganciclovir, Valganciclovir, and Other Drugs that Undergo Renal Tubular Secretion: May increase concentrations of mycophenolic acid glucuronide (MPAG) and coadministered drug; monitor blood cell counts. ( 7.9)
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Dosage in Adult Kidney Transplant Patients
The recommended dose of mycophenolic acid delayed-release tablets is 720 mg administered twice daily (1,440 mg total daily dose).
2.2 Dosage in Pediatric Kidney Transplant Patients
The recommended dose of mycophenolic acid delayed-release tablets in conversion (at least 6 months post-transplant) pediatric patients age 5 years and older is 400 mg/m 2 body surface area (BSA) administered twice daily (up to a maximum dose of 720 mg administered twice daily).
2.3 Administration
Mycophenolic acid delayed-release tablets should be taken on an empty stomach, 1 hour before or 2 hours after food intake [ see Clinical Pharmacology (12.3)].
Mycophenolic acid delayed-release tablets should not be crushed, chewed, or cut prior to ingesting. The tablets should be swallowed whole in order to maintain the integrity of the enteric coating.
Pediatric patients with a BSA of 1.19 m 2 to 1.58 m 2 may be dosed either with three mycophenolic acid delayed-release 180 mg tablets, or one 180 mg tablet plus one 360 mg tablet twice daily (1,080 mg daily dose). Patients with a BSA of >1.58 m 2 may be dosed either with four mycophenolic acid delayed-release 180 mg tablets, or two mycophenolic acid delayed-release 360 mg tablets twice daily (1,440 mg daily dose). Pediatric doses for patients with BSA <1.19 m 2 cannot be accurately administered using currently available formulations of mycophenolic acid delayed-release tablets.
- In adults: 720 mg by mouth, twice daily (1,440 mg total daily dose) on an empty stomach, 1 hour before or 2 hours after food intake. ( 2.1)
- In children: 5 years of age and older (who are at least 6 months post kidney transplant), 400 mg/m 2 by mouth, twice daily (up to a maximum of 720 mg twice daily). ( 2.2)
- Do not crush, chew, or cut tablet prior to ingestion. ( 2.3)
DOSAGE FORMS & STRENGTHS SECTION
3 DOSAGE FORMS AND STRENGTHS
Mycophenolic acid delayed-release tablets, USP, are available as 360 mg and 180 mg tablets.
Table 1: Description of Mycophenolic Acid Delayed-Release Tablets|
Dosage Strength |
360 mg tablet |
180 mg tablet |
|
Active ingredient |
mycophenolic acid as mycophenolate sodium |
mycophenolic acid as mycophenolate sodium |
|
Appearance |
Orange-red film-coated oval tablet |
White film-coated round tablet |
|
Debossing/Imprint |
“T161” debossed on one side |
“T160” imprinted on one side |
Mycophenolic acid delayed-release tablets are available as 180 mg and 360 mg tablets. ( 3)
DESCRIPTION SECTION
11 DESCRIPTION
Mmycophenolic acid delayed-release tablets, USP are an enteric formulation of mycophenolate sodium that delivers the active moiety mycophenolic acid (MPA). Mycophenolic acid is an immunosuppressive agent. As the sodium salt, MPA is chemically designated as (E)-6-(4-hydroxy-6-methoxy-7-methyl-3-oxo-1,3-dihydroisobenzofuran-5-yl)-4-methylhex-4-enoic acid sodium salt.
Its empirical formula is C 17H 19O 6Na. The molecular weight is 342.32 g/mol and the structural formula is:
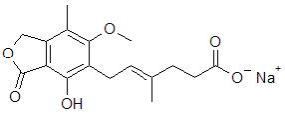
Mycophenolic acid, USP as the sodium salt, is a white to off-white, crystalline powder and is highly soluble in aqueous media at physiological pH and practically insoluble in 0.1N hydrochloric acid.
Mycophenolic acid is available for oral use as delayed-release tablets containing either 180 mg or 360 mg of mycophenolic acid. Inactive ingredients include crospovidone, hypromellose, lactose anhydrous, magnesium stearate, povidone, and starch. The enteric coating of the tablet consists of hypromellose phthalate, titanium dioxide, triethyl citrate, ferrosoferric oxide (180 mg), lactose monohydrate (180 mg), propylene glycol (180 mg) and triacetin (180 mg) or polyethylene glycol (360 mg), talc (360 mg), and FD&C yellow # 6 aluminum lake (360 mg).
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
360 mg tablet: Orange, film-coated ovaloid tablet with “T161” debossed on one side, containing 360 mg mycophenolic acid (MPA) as mycophenolate sodium.
Bottles of 120…………………………………………………………………NDC 72789-246-98
180 mg tablet: White, film-coated round tablet and “T160” imprinted on one side, containing 180 mg mycophenolic acid (MPA) as mycophenolate sodium.
Bottles of 120…………………………………………………………………NDC 72789-247-98
Storage
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C and 30°C (59°F and 86°F) [see USP Controlled Room Temperature]. Protect from moisture.Dispense in a tight container (USP).
Handling
Keep out of reach and sight of children. Mycophenolic acid delayed-release tablets should not be crushed or cut in order to maintain the integrity of the enteric coating [ see Dosage and Administration (2.3)].
Teratogenic effects have been observed with mycophenolate sodium [ see Warnings and Precautions (5.1)]. If for any reason the mycophenolic acid delayed-release tablets must be crushed, avoid inhalation of the powder, or direct contact of the powder, with skin or mucous membranes.