
Sildenafil
These highlights do not include all the information needed to use SILDENAFIL TABLETS safely and effectively. See full prescribing information for SILDENAFIL TABLETS. SILDENAFIL tablets, for oral use Initial U.S. Approval: 1998
d35f8d6b-e642-78bb-e053-2995a90abb2e
HUMAN PRESCRIPTION DRUG LABEL
Jul 14, 2023
NuCare Pharmaceuticals,Inc.
DUNS: 010632300
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Sildenafil
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (10)
Drug Labeling Information
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
Sildenafil tablets, USP are indicated for the treatment of pulmonary arterial hypertension (WHO Group I) in adults to improve exercise ability and delay clinical worsening. The delay in clinical worsening was demonstrated when sildenafil tablets was added to background epoprostenol therapy [see Clinical Studies ( 14)].
Studies establishing effectiveness were short-term (12 to 16 weeks), and included predominately patients with New York Heart Association (NYHA) Functional Class II-III symptoms and idiopathic etiology (71%) or associated with connective tissue disease (CTD) (25%).
Limitation of Use: Adding sildenafil to bosentan therapy does not result in any beneficial effect on exercise capacity [see Clinical Studies ( 14)].
WARNINGS AND PRECAUTIONS SECTION
5 WARNINGS AND PRECAUTIONS
5.1 Mortality with Pediatric Use
In a long-term trial in pediatric patients with PAH, an increase in mortality with increasing sildenafil tablets dose was observed. Deaths were first observed after about 1 year and causes of death were typical of patients with PAH. Use of sildenafil tablets, particularly chronic use, is not recommended in children [see Use in Specific Populations ( 8.4)].
5.2 Hypotension
Sildenafil tablets has vasodilatory properties, resulting in mild and transient decreases in blood pressure. Before prescribing sildenafil tablets, carefully consider whether patients with certain underlying conditions could be adversely affected by such vasodilatory effects (e.g., patients on antihypertensive therapy or with resting hypotension [BP less than 90/50], fluid depletion, severe left ventricular outflow obstruction, or autonomic dysfunction). Monitor blood pressure when co-administering blood pressure lowering drugs with sildenafil tablets.
5.3 Worsening Pulmonary Vascular Occlusive Disease
Pulmonary vasodilators may significantly worsen the cardiovascular status of patients with pulmonary venoocclusive disease (PVOD). Since there are no clinical data on administration of sildenafil tablets to patients with venoocclusive disease, administration of sildenafil tablets to such patients is not recommended. Should signs of pulmonary edema occur when sildenafil tablets is administered, consider the possibility of associated PVOD.
5.4 Epistaxis
The incidence of epistaxis was 13% in patients taking sildenafil tablets with PAH secondary to CTD. This effect was not seen in idiopathic PAH (Sildenafil tablets 3%, placebo 2%) patients. The incidence of epistaxis was also higher in sildenafil tablets-treated patients with a concomitant oral vitamin K antagonist (9% versus 2% in those not treated with concomitant vitamin K antagonist).
The safety of sildenafil tablets is unknown in patients with bleeding disorders or active peptic ulceration.
5.5 Visual Loss
When used to treat erectile dysfunction, non-arteritic anterior ischemic optic neuropathy (NAION), a cause of decreased vision including permanent loss of vision, has been reported postmarketing in temporal association with the use of phosphodiesterase type 5 (PDE-5) inhibitors, including sildenafil. Most, but not all, of these patients had underlying anatomic or vascular risk factors for developing NAION, including but not necessarily limited to: low cup to disc ratio (“crowded disc”), age over 50, diabetes, hypertension, coronary artery disease, hyperlipidemia and smoking. Based on published literature, the annual incidence of NAION is 2.5-11.8 cases per 100,000 males aged ≥ 50 per year in the general population. An observational case-crossover study evaluated the risk of NAION when PDE-5 inhibitor use, as a class, occurred immediately before NAION onset (within 5 half-lives), compared to PDE-5 inhibitor use in a prior time period. The results suggest an approximate 2-fold increase in the risk of NAION, with a risk estimate of 2.15 (95% CI 1.06, 4.34). A similar study reported a consistent result, with a risk estimate of 2.27 (95% CI 0.99, 5.20). Other risk factors for NAION, such as the presence of “crowded” optic disc, may have contributed to the occurrence of NAION in these studies.
Neither the rare postmarketing reports, nor the association of PDE-5 inhibitor use and NAION in the observational studies, substantiate a causal relationship between PDE-5 inhibitor use and NAION [see Adverse Reactions ( 6.2] .
Advise patients to seek immediate medical attention in the event of a sudden loss of vision in one or both eyes while taking PDE-5 inhibitors, including sildenafil tablets. Physicians should also discuss the increased risk of NAION with patients who have already experienced NAION in one eye, including whether such individuals could be adversely affected by use of vasodilators, such as PDE-5 inhibitors.
There are no controlled clinical data on the safety or efficacy of sildenafil tablets in patients with retinitis pigmentosa, a minority whom have genetic disorders of retinal phosphodiesterases. Prescribe sildenafil tablets with caution in these patients.
5.6 Hearing Loss
Cases of sudden decrease or loss of hearing, which may be accompanied by tinnitus and dizziness, have been reported in temporal association with the use of PDE-5 inhibitors, including sildenafil tablets. In some of the cases, medical conditions and other factors were reported that may have played a role. In many cases, medical follow-up information was limited. It is not possible to determine whether these reported events are related directly to the use of sildenafil tablets, to the patient’s underlying risk factors for hearing loss, a combination of these factors, or to other factors.
Advise patients to seek prompt medical attention in the event of sudden decrease or loss of hearing while taking PDE-5 inhibitors, including sildenafil tablets.
5.7 Combination with other PDE-5 Inhibitors
Sildenafil is also marketed as VIAGRA ®. The safety and efficacy of combinations of sildenafil tablets with VIAGRA or other PDE-5 inhibitors have not been studied. Inform patients taking sildenafil tablets not to take VIAGRA or other PDE-5 inhibitors.
5.8 Priapism
Use sildenafil tablets with caution in patients with anatomical deformation of the penis (e.g., angulation, cavernosal fibrosis, or Peyronie’s disease) or in patients who have conditions, which may predispose them to priapism (e.g., sickle cell anemia, multiple myeloma, or leukemia). In the event of an erection that persists longer than 4 hours, the patient should seek immediate medical assistance. If priapism (painful erection greater than 6 hours in duration) is not treated immediately, penile tissue damage and permanent loss of potency could result.
5.9 Vaso-occlusive Crisis in Patients with Pulmonary Hypertension Secondary
to Sickle Cell Anemia
In a small, prematurely terminated study of patients with pulmonary hypertension (PH) secondary to sickle cell disease, vaso-occlusive crises requiring hospitalization were more commonly reported by patients who received sildenafil tablets than by those randomized to placebo. The effectiveness and safety of sildenafil tablets in the treatment of PAH secondary to sickle cell anemia has not been established.
- Increased mortality with increasing doses in pediatric patients. Not recommended for use in pediatric patients. ( 5.1)
- Vasodilation effects may be more common in patients with hypotension or on antihypertensive therapy. ( 5.2)
- Use in pulmonary veno-occlusive disease may cause pulmonary edema and is not recommended. ( 5.3)
- Hearing or visual impairment: Seek medical attention if sudden decrease or loss of vision or hearing occurs. ( 5.5, 5.6)
- Pulmonary hypertension secondary to sickle cell disease: Sildenafil tablets may cause serious vaso-occlusive crises. ( 5.9)
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Limited published data from randomized controlled trials, case-controlled trials, and case series do not report a clear association with sildenafil and major birth defects, miscarriage, or adverse maternal or fetal outcomes when sildenafil is used during pregnancy. There are risks to the mother and fetus from untreated pulmonary arterial hypertension (see Clinical Considerations). Animal reproduction studies conducted with sildenafil showed no evidence of embryo-fetal toxicity or teratogenicity at doses up to 32- and 65-times the recommended human dose (RHD) of 20 mg three times a day in rats and rabbits, respectively (See Data).
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
Pregnant women with untreated pulmonary arterial hypertension are at risk for heart failure, stroke, preterm delivery, and maternal and fetal death.
Data
Animal Data
No evidence of teratogenicity, embryotoxicity, or fetotoxicity was observed in
pregnant rats or rabbits dosed with sildenafil 200 mg/kg/day during
organogenesis, a level that is, on a mg/m 2 basis, 32- and 65-times,
respectively, the recommended human dose (RHD) of 20 mg three times a day. In
a rat pre-and postnatal development study, the no-observed-adverse-effect dose
was 30 mg/kg/day (equivalent to 5-times the RHD on a mg/m 2 basis).
8.2 Lactation
Risk Summary
Limited published data from a case report describe the presence of sildenafil and its active metabolite in human milk. There is insufficient information about the effects of sildenafil on the breastfed infant and no information on the effects of sildenafil on milk production. Limited clinical data during lactation preclude a clear determination of the risk of sildenafil tablets to an infant during lactation.
8.4 Pediatric Use
In a randomized, double-blind, multi-center, placebo-controlled, parallel- group, dose-ranging study, 234 patients with PAH, aged 1 to 17 years, body weight greater than or equal to 8 kg, were randomized, on the basis of body weight, to three dose levels of sildenafil tablets, or placebo, for 16 weeks of treatment. Most patients had mild to moderate symptoms at baseline: WHO Functional Class I (32%), II (51%), III (15%), or IV (0.4%). One-third of patients had primary PAH; two-thirds had secondary PAH (systemic-to-pulmonary shunt in 37%; surgical repair in 30%). Sixty-two percent of patients were female. Drug or placebo was administered three times a day.
The primary objective of the study was to assess the effect of sildenafil tablets on exercise capacity as measured by cardiopulmonary exercise testing in pediatric patients developmentally able to perform the test (n = 115). Administration of sildenafil tablets did not result in a statistically significant improvement in exercise capacity in those patients. No patients died during the 16-week controlled study.
After completing the 16-week controlled study, a patient originally randomized to sildenafil tablets remained on his/her dose of sildenafil tablets or, if originally randomized to placebo, was randomized to low-, medium-, or high- dose sildenafil tablets. After all patients completed 16 weeks of follow-up in the controlled study, the blind was broken and doses were adjusted as clinically indicated. Patients treated with sildenafil were followed for a median of 4.6 years (range 2 days to 8.6 years). Mortality during the long- term study, by originally assigned dose, is shown in Figure 1:
Figure 1: Kaplan-Meier Plot of Mortality by Sildenafil tablets Dose
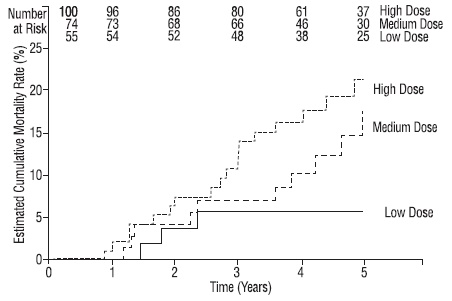
During the study, there were 42 reported deaths, with 37 of these deaths reported prior to a decision to titrate subjects to a lower dosage because of a finding of increased mortality with increasing sildenafil tablets doses. For the survival analysis which included 37 deaths, the hazard ratio for high dose compared to low dose was 3.9, p=0.007. Causes of death were typical of patients with PAH. Use of sildenafil tablets, particularly chronic use, is not recommended in children.
8.5 Geriatric Use
Clinical studies of sildenafil tablets did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy [see Clinical Pharmacology ( 12.3)].
8.6 Patients with Hepatic Impairment
No dose adjustment for mild to moderate impairment is required. Severe impairment has not been studied [see Clinical Pharmacology ( 12.3)].
8.7 Patients with Renal Impairment
No dose adjustment is required (including severe impairment CLcr < 30 mL/min) [see Clinical Pharmacology ( 12.3)].
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Sildenafil was not carcinogenic when administered to rats for up to 24 months at 60 mg/kg/day, a dose resulting in total systemic exposure (AUC) to unbound sildenafil and its major metabolite 33- and 37- times, for male and female rats respectively, the human exposure at the RHD of 20 mg three times a day. Sildenafil was not carcinogenic when administered to male and female mice for up to 21 and 18 months, respectively, at doses up to a maximally tolerated level of 10 mg/kg/day, a dose equivalent to the RHD on a mg/m 2 basis.
Sildenafil was negative in in vitro bacterial and Chinese hamster ovary cell assays to detect mutagenicity, and in vitro human lymphocytes and in vivo mouse micronucleus assays to detect clastogenicity.
There was no impairment of fertility in male or female rats given up to 60 mg sildenafil/kg/day, a dose producing a total systemic exposure (AUC) to unbound sildenafil and its major metabolite of 19- and 38- times for males and females, respectively, the human exposure at the RHD of 20 mg three times a day.
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
Studies of Adults with Pulmonary Arterial Hypertension
Study 1 (Sildenafil tablets monotherapy (20 mg, 40 mg, and 80 mg three times a day))
A randomized, double-blind, placebo-controlled study of sildenafil tablets (Study 1) was conducted in 277 patients with PAH (defined as a mean pulmonary artery pressure of greater than or equal to 25 mmHg at rest with a pulmonary capillary wedge pressure less than 15 mmHg). Patients were predominantly World Health Organization (WHO) functional classes II-III. Allowed background therapy included a combination of anticoagulants, digoxin, calcium channel blockers, diuretics, and oxygen. The use of prostacyclin analogues, endothelin receptor antagonists, and arginine supplementation were not permitted. Subjects who had failed to respond to bosentan were also excluded. Patients with left ventricular ejection fraction less than 45% or left ventricular shortening fraction less than 0.2 also were not studied.
Patients were randomized to receive placebo (n=70) or sildenafil tablets 20 mg (n = 69), 40 mg (n = 67) or 80 mg (n = 71) three times a day for a period of 12 weeks. They had either primary pulmonary hypertension (PPH) (63%), PAH associated with CTD (30%), or PAH following surgical repair of left-to-right congenital heart lesions (7%). The study population consisted of 25% men and 75% women with a mean age of 49 years (range: 18-81 years) and baseline 6-minute walk distance between 100 and 450 meters (mean 343).
The primary efficacy endpoint was the change from baseline at week 12 (at least 4 hours after the last dose) in the 6-minute walk distance. Placebo- corrected mean increases in walk distance of 45-50 meters were observed with all doses of sildenafil tablets. These increases were significantly different from placebo, but the sildenafil tablets dose groups were not different from each other (see Figure 4), indicating no additional clinical benefit from doses higher than 20 mg three times a day. The improvement in walk distance was apparent after 4 weeks of treatment and was maintained at week 8 and week 12.
Figure 4. Change from Baseline in 6-Minute Walk Distance (meters) at Weeks 4, 8, and 12 in Study 1: Mean (95% Confidence Interval)
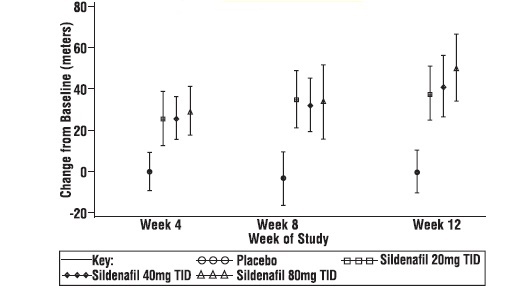
Figure 5 displays subgroup efficacy analyses in Study 1 for the change from
baseline in 6-Minute Walk Distance at Week 12 including baseline walk
distance, disease etiology, functional class, gender, age, and hemodynamic
parameters.
Figure 5. Placebo-Corrected Change From Baseline in 6-Minute Walk Distance (meters) at Week 12 by study subpopulation in Study 1: Mean (95% Confidence Interval)
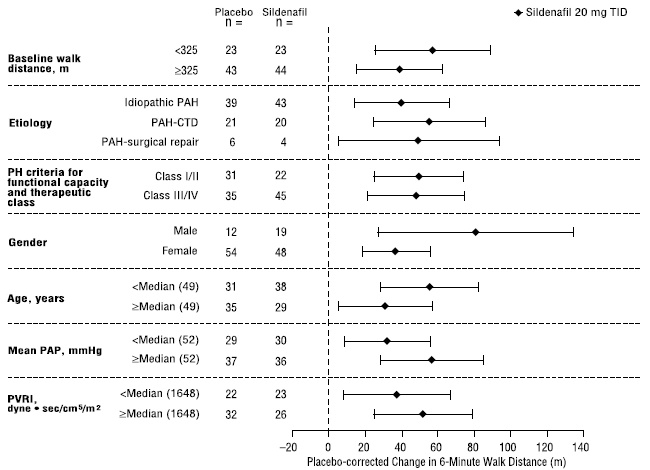
Key: PAH = pulmonary arterial hypertension; CTD = connective tissue disease; PH = pulmonary hypertension; PAP = pulmonary arterial pressure; PVRI = pulmonary vascular resistance index; TID = three times daily.
Of the 277 treated patients, 259 entered a long-term, uncontrolled extension study. At the end of 1 year, 94% of these patients were still alive. Additionally, walk distance and functional class status appeared to be stable in patients taking sildenafil tablets. Without a control group, these data must be interpreted cautiously.
Study 2 (Sildenafil tablets co-administered with epoprostenol)
A randomized, double-blind, placebo controlled study (Study 2) was conducted in 267 patients with PAH who were taking stable doses of intravenous epoprostenol. Patients had to have a mean pulmonary artery pressure (mPAP) greater than or equal to 25 mmHg and a pulmonary capillary wedge pressure (PCWP) less than or equal to 15 mmHg at rest via right heart catheterization within 21 days before randomization, and a baseline 6-minute walk test distance greater than or equal to 100 meters and less than or equal to 450 meters (mean 349 meters). Patients were randomized to placebo or sildenafil tablets (in a fixed titration starting from 20 mg, to 40 mg and then 80 mg, three times a day) and all patients continued intravenous epoprostenol therapy.
At baseline patients had PPH (80%) or PAH secondary to CTD (20%);WHO functional class I (1%), II (26%), III (67%), or IV (6%); and the mean age was 48 years, 80% were female, and 79% were Caucasian.
There was a statistically significant greater increase from baseline in 6-minute walk distance at Week 16 (primary endpoint) for the sildenafil tablets group compared with the placebo group. The mean change from baseline at Week 16 (last observation carried forward) was 30 meters for the sildenafil tablets group compared with 4 meters for the placebo group giving an adjusted treatment difference of 26 meters (95% CI: 10.8, 41.2) (p = 0.0009).
Patients on sildenafil tablets achieved a statistically significant reduction in mPAP compared to those on placebo. A mean placebo-corrected treatment effect of -3.9 mmHg was observed in favor of sildenafil tablets (95% CI: -5.7, -2.1) (p = 0.00003).
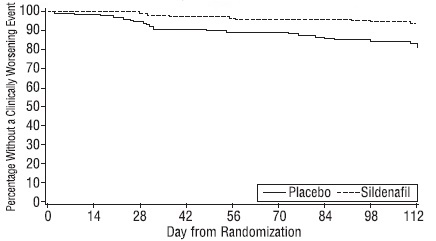
Time to clinical worsening of PAH was defined as the time from randomization to the first occurrence of a clinical worsening event (death, lung transplantation, initiation of bosentan therapy, or clinical deterioration requiring a change in epoprostenol therapy). Table 4 displays the number of patients with clinical worsening events in Study 2. Kaplan-Meier estimates and a stratified log-rank test demonstrated that placebo-treated patients were 3 times more likely to experience a clinical worsening event than sildenafil tablets-treated patients and that sildenafil tablets -treated patients experienced a significant delay in time to clinical worsening versus placebo- treated patients (p = 0.0074). Kaplan-Meier plot of time to clinical worsening is presented in Figure 6.
Table 4. Clinical Worsening Events in Study 2|
Placebo |
Sildenafil tablets | |||
|
Number of subjects with clinical worsening first event |
23 |
8 | ||
|
First Event |
All Events |
First Event |
All Events | |
|
Death, n |
3 |
4 |
0 |
0 |
|
Lung Transplantation, n |
1 |
1 |
0 |
0 |
|
Hospitalization due to PAH, n |
9 |
11 |
8 |
8 |
|
Clinical deterioration resulting in: |
9 |
16 |
0 |
2 |
|
Proportion Worsened |
0.187 |
0.062 |
Figure 6. Kaplan-Meier Plot of Time (in Days) to Clinical Worsening of PAH in Study 2
Improvements in WHO functional class for PAH were also demonstrated in
subjects on sildenafil tablets compared to placebo. More than twice as many
sildenafil tablets-treated patients (36%) as placebo-treated patients (14%)
showed an improvement in at least one functional New York Heart Association
(NYHA) class for PAH.
Study 3 (Sildenafil tablets monotherapy (1 mg, 5 mg, and 20 mg three times a day))
A randomized, double-blind, parallel dose study (Study 3) was planned in 219 patients with PAH. This study was prematurely terminated with 129 subjects enrolled. Patients were required to have a mPAP greater than or equal to 25 mmHg and a PCWP less than or equal to 15 mmHg at rest via right heart catheterization within 12 weeks before randomization, and a baseline 6-minute walk test distance greater than or equal to 100 meters and less than or equal to 450 meters (mean 345 meters). Patients were randomized to 1 of 3 doses of sildenafil tablets: 1 mg, 5 mg, and 20 mg, three times a day.
At baseline patients had PPH (74%) or secondary PAH (26%); WHO functional class II (57%), III (41%), or IV (2%); the mean age was 44 years; and 67% were female. The majority of subjects were Asian (67%), and 28% were Caucasian.
The primary efficacy endpoint was the change from baseline at Week 12 (at least 4 hours after the last dose) in the 6-minute walk distance. Similar increases in walk distance (mean increase of 38-41 meters) were observed in the 5 and 20 mg dose groups. These increases were significantly better than those observed in the 1 mg dose group (Figure 7).
Figure 7. Mean Change from Baseline in Six Minute Walk (meters) by Visit to Week 12 – ITT Population Sildenafil Protocol A1481244

Study 4 (Sildenafil tablets added to bosentan therapy – lack of effect on exercise capacity)
A randomized, double-blind, placebo controlled study was conducted in 103 patients with PAH who were on bosentan therapy for a minimum of three months. The PAH patients included those with primary PAH, and PAH associated with CTD. Patients were randomized to placebo or sildenafil (20 mg three times a day) in combination with bosentan (62.5-125 mg twice a day). The primary efficacy endpoint was the change from baseline at Week 12 in 6MWD. The results indicate that there is no significant difference in mean change from baseline on 6MWD observed between sildenafil 20 mg plus bosentan and bosentan alone.