
NULOJIX
These highlights do not include all the information needed to use NULOJIX safely and effectively. See full prescribing information for NULOJIX. NULOJIX (belatacept) for injection, for intravenous useInitial U.S. Approval: 2011
c16ac648-d5d2-9f7d-8637-e2328572754e
HUMAN PRESCRIPTION DRUG LABEL
Jul 28, 2021
E.R. Squibb & Sons, L.L.C.
DUNS: 011550092
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
BELATACEPT
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (4)
Drug Labeling Information
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
1.1 Adult Kidney Transplant Recipients
NULOJIX® (belatacept) is indicated for prophylaxis of organ rejection in adult patients receiving a kidney transplant. NULOJIX is to be used in combination with basiliximab induction, mycophenolate mofetil, and corticosteroids.
1.2 Limitations of Use
Use NULOJIX only in patients who are EBV seropositive [see Contraindications (4) and Warnings and Precautions (5.1)].
Use of NULOJIX for the prophylaxis of organ rejection in transplanted organs other than kidney has not been established [see Warnings and Precautions (5.6)].
•
NULOJIX is a selective T cell costimulation blocker indicated for prophylaxis of organ rejection in adult patients receiving a kidney transplant. (1.1)
•
Use in combination with basiliximab induction, mycophenolate mofetil, and corticosteroids. (1.1)
Limitations of Use:
•
Use only in patients who are EBV seropositive. (1.2, 4, 5.1)
•
Use has not been established for the prophylaxis of organ rejection in transplanted organs other than the kidney. (1.2, 5.6)
CONTRAINDICATIONS SECTION
4 CONTRAINDICATIONS
NULOJIX is contraindicated in transplant recipients who are Epstein-Barr virus (EBV) seronegative or with unknown EBV serostatus due to the risk of post- transplant lymphoproliferative disorder (PTLD), predominantly involving the central nervous system (CNS) [see Boxed Warning and Warnings and Precautions (5.1)].
Patients who are EBV seronegative or with unknown EBV serostatus. (4)
WARNINGS AND PRECAUTIONS SECTION
5 WARNINGS AND PRECAUTIONS
5.1 Post-Transplant Lymphoproliferative Disorder
NULOJIX-treated patients have an increased risk for developing post-transplant lymphoproliferative disorder (PTLD), predominantly involving the CNS, compared to patients on a cyclosporine-based regimen [see Adverse Reactions (6.1), Clinical Studies (14.2)]. As the total burden of immunosuppression is a risk factor for PTLD, higher than the recommended doses or more frequent dosing of NULOJIX and higher than recommended doses of concomitant immunosuppressive agents are not recommended [see Dosage and Administration (2.1) and Warnings and Precautions (5.6)]. Physicians should consider PTLD in patients reporting new or worsening neurological, cognitive, or behavioral signs or symptoms.
EBV Serostatus
The risk of PTLD was higher in EBV seronegative patients compared to EBV seropositive patients. EBV seropositive patients are defined as having evidence of acquired immunity shown by the presence of IgG antibodies to viral capsid antigen (VCA) and EBV nuclear antigen (EBNA).
Epstein-Barr virus serology should be ascertained before starting administration of NULOJIX, and only patients who are EBV seropositive should receive NULOJIX. Transplant recipients who are EBV seronegative, or with unknown serostatus, should not receive NULOJIX [see Boxed Warning and Contraindications (4)].
Other Risk Factors
Other known risk factors for PTLD include cytomegalovirus (CMV) infection and T cell-depleting therapy. T cell-depleting therapies to treat acute rejection should be used cautiously. CMV prophylaxis is recommended for at least 3 months after transplantation [see Warnings and Precautions (5.5)].
Patients who are EBV seropositive and CMV seronegative may be at increased risk for PTLD compared to patients who are EBV seropositive and CMV seropositive [see Adverse Reactions (6.1)]. Since CMV seronegative patients are at increased risk for CMV disease (a known risk factor for PTLD), the clinical significance of CMV serology for PTLD remains to be determined; however, these findings should be considered when prescribing NULOJIX.
5.2 Management of Immunosuppression
Only physicians experienced in management of systemic immunosuppressant therapy in transplantation should prescribe NULOJIX. Patients receiving the drug should be managed in facilities equipped and staffed with adequate laboratory and supportive medical resources. The physician responsible for the maintenance therapy should have complete information requisite for the follow- up of the patient [see Boxed Warning].
5.3 Other Malignancies
Patients receiving immunosuppressants, including NULOJIX, are at increased risk of developing malignancies, in addition to PTLD, including the skin [see Boxed Warning and Warnings and Precautions (5.1)]. Exposure to sunlight and ultraviolet (UV) light should be limited by wearing protective clothing and using a sunscreen with a high protection factor.
5.4 Progressive Multifocal Leukoencephalopathy
Progressive multifocal leukoencephalopathy (PML) is an often rapidly progressive and fatal opportunistic infection of the CNS that is caused by the JC virus, a human polyoma virus. In clinical trials with NULOJIX, two cases of PML were reported in patients receiving NULOJIX at higher cumulative doses and more frequently than the recommended regimen, along with mycophenolate mofetil (MMF) and corticosteroids; one case occurred in a kidney transplant recipient and the second case occurred in a liver transplant recipient [see Warnings and Precautions (5.6), Adverse Reactions (6.1), Clinical Studies (14.2)]. As PML has been associated with high levels of overall immunosuppression, the recommended doses and frequency of NULOJIX and concomitant immunosuppressives, including MMF, should not be exceeded.
Physicians should consider PML in the differential diagnosis in patients with new or worsening neurological, cognitive, or behavioral signs or symptoms. PML is usually diagnosed by brain imaging, cerebrospinal fluid (CSF) testing for JC viral DNA by polymerase chain reaction (PCR), and/or brain biopsy. Consultation with a specialist (eg, neurologist and/or infectious disease) should be considered for any suspected or confirmed cases of PML.
If PML is diagnosed, consideration should be given to reduction or withdrawal of immunosuppression taking into account the risk to the allograft.
5.5 Other Serious Infections
Patients receiving immunosuppressants, including NULOJIX, are at increased risk of developing bacterial, viral (cytomegalovirus [CMV] and herpes), fungal, and protozoal infections, including opportunistic infections. These infections may lead to serious, including fatal, outcomes [see Boxed Warning and Adverse Reactions (6.1)].
Prophylaxis for cytomegalovirus is recommended for at least 3 months after transplantation. Prophylaxis for Pneumocystis jiroveci is recommended after transplantation.
Tuberculosis
Tuberculosis was more frequently observed in patients receiving NULOJIX than cyclosporine in clinical trials [see Adverse Reactions (6.1)]. Patients should be evaluated for tuberculosis and tested for latent infection prior to initiating NULOJIX. Treatment of latent tuberculosis infection should be initiated prior to NULOJIX use.
Polyoma Virus Nephropathy
In addition to cases of JC virus-associated PML [see Warnings and Precautions (5.4)], cases of polyoma virus-associated nephropathy (PVAN), mostly due to BK virus infection, have been reported. PVAN is associated with serious outcomes; including deteriorating renal function and kidney graft loss [see Adverse Reactions (6.1)]. Patient monitoring may help detect patients at risk for PVAN. Reductions in immunosuppression should be considered for patients who develop evidence of PVAN. Physicians should also consider the risk that reduced immunosuppression represents to the functioning allograft.
5.6 Liver Transplant
Use of NULOJIX in liver transplant patients is not recommended [see Boxed Warning]. In a clinical trial of liver transplant patients, use of NULOJIX regimens with more frequent administration of belatacept than any of those studied in kidney transplant, along with mycophenolate mofetil (MMF) and corticosteroids, was associated with a higher rate of graft loss and death compared to the tacrolimus control arms. In addition, two cases of PTLD involving the liver allograft (one fatal) and one fatal case of PML were observed among the 147 patients randomized to NULOJIX. The two cases of PTLD were reported among the 140 EBV seropositive patients (1.4%). The fatal case of PML was reported in a patient receiving higher than recommended doses of NULOJIX and MMF [see Warnings and Precautions (5.4)].
5.7 Acute Rejection and Graft Loss with Corticosteroid Minimization
In postmarketing experience, use of NULOJIX in conjunction with basiliximab induction, MMF, and corticosteroid minimization to 5 mg per day between Day 3 and Week 6 post-transplant was associated with an increased rate and grade of acute rejection, particularly Grade III rejection. These Grade III rejections occurred in patients with 4 to 6 HLA mismatches. Graft loss was a consequence of Grade III rejection in some patients.
Corticosteroid utilization should be consistent with the NULOJIX clinical trial experience [see Dosage and Administration (2.1) and Clinical Studies (14.1)].
5.8 Immunizations
The use of live vaccines should be avoided during treatment with NULOJIX, including but not limited to the following: intranasal influenza, measles, mumps, rubella, oral polio, BCG, yellow fever, varicella, and TY21a typhoid vaccines.
5.9 Coadministration with Anti-Thymocyte Globulin
In postmarketing experience in de novo kidney transplant recipients, some with other predisposing risk factors for venous thrombosis of the renal allograft, venous thrombosis of the renal allograft has occurred when the initial dose of anti-thymocyte globulin, as immunosuppressive induction, was coadministered (at the same or nearly the same time) with the first dose of belatacept. In such patients, the coadministration (at the same or nearly the same time) of anti-thymocyte globulin and belatacept may pose a risk for venous thrombosis of the renal allograft. If anti-thymocyte globulin (or any other cell- depleting induction treatment) and belatacept will be administered concomitantly, a twelve-hour interval between the two administrations is suggested.
5.10 Risk of Rejection with Conversion From a CNI Based Maintenance
Regimen
Conversion of patients receiving a CNI based maintenance regimen to a NULOJIX based maintenance regimen increases the risk of acute rejection. In two randomized controlled studies, kidney transplant recipients at least six months post-transplant and stable on a CNI based regimen who were converted to a belatacept based regimen experienced higher rejection rates mostly during the first year post-conversion than patients maintained on their CNI based regimens. Conversion of stable kidney transplant recipients from a CNI based maintenance therapy to a belatacept based maintenance therapy is not recommended unless the patient is CNI intolerant.
•
Post-Transplant Lymphoproliferative Disorder (PTLD): increased risk, predominantly involving the CNS; monitor for new or worsening neurological, cognitive, or behavioral signs and symptoms. (Boxed Warning, 4, 5.1, 5.6)
•
Other malignancies: increased risk with all immunosuppressants; appears related to intensity and duration of use. Avoid prolonged exposure to UV light and sunlight. (5.3)
•
Progressive Multifocal Leukoencephalopathy (PML): increased risk; consider in the diagnosis of patients reporting new or worsening neurological, cognitive, or behavioral signs and symptoms. Recommended doses of immunosuppressants should not be exceeded. (5.4)
•
Other serious infections: increased risk of bacterial, viral, fungal, and protozoal infections, including opportunistic infections and tuberculosis. Some infections were fatal. Polyoma virus-associated nephropathy can lead to kidney graft loss; consider reduction in immunosuppression. Evaluate for tuberculosis and initiate treatment for latent infection prior to NULOJIX use. Cytomegalovirus and pneumocystis prophylaxis are recommended after transplantation. (5.1, 5.4, 5.5)
•
Liver transplant: use is not recommended. (5.6)
•
Acute Rejection and Graft Loss with Corticosteroid Minimization: corticosteroid utilization should be consistent with the NULOJIX clinical trial experience. (2.1, 5.7, 14.1)
•
Immunizations: avoid use of live vaccines during treatment. (5.8)
•
Coadministration with Anti-Thymocyte Globulin: in de novo kidney transplant recipients, especially those with other predisposing risk factors for venous thrombosis of the renal allograft, coadministration (at the same or nearly the same time) with anti-thymocyte globulin may pose a risk for venous thrombosis of the renal allograft. (5.9, 6.2, 7.3)
•
Risk of Rejection with Conversion From a CNI Based Maintenance Regimen: conversion of maintenance kidney transplant recipients from a CNI based to NULOJIX based maintenance regimen increases the risk of acute rejection. Conversion of stable kidney transplant recipients from a CNI based maintenance therapy to a belatacept based maintenance therapy is not recommended unless the patient is CNI intolerant. (5.10)
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Dosage in Adult Kidney Transplant Recipients
NULOJIX should be administered in combination with basiliximab induction, mycophenolate mofetil (MMF), and corticosteroids. In clinical trials the median (25th to 75th percentile) corticosteroid doses were tapered to approximately 15 mg (10 to 20 mg) per day by the first 6 weeks and remained at approximately 10 mg (5 to 10 mg) per day for the first 6 months post- transplant. Corticosteroid utilization should be consistent with the NULOJIX clinical trial experience [see Warnings and Precautions (5.7) and Clinical Studies (14.1)].
Due to an increased risk of post-transplant lymphoproliferative disorder (PTLD) predominantly involving the central nervous system (CNS), progressive multifocal leukoencephalopathy (PML), and serious CNS infections, administration of higher than the recommended doses or more frequent dosing of NULOJIX is not recommended [see Warnings and Precautions (5.1, 5.4, 5.5) and Adverse Reactions (6.1)].
NULOJIX is for intravenous infusion only. Patients do not require premedication prior to administration of NULOJIX.
Dosing instructions are provided in Table 1.
•
The total infusion dose of NULOJIX should be based on the actual body weight of the patient at the time of transplantation, and should not be modified during the course of therapy, unless there is a change in body weight of greater than 10%.
•
The prescribed dose of NULOJIX must be evenly divisible by 12.5 mg in order for the dose to be prepared accurately using the reconstituted solution and the silicone-free disposable syringe provided. Evenly divisible increments are 0, 12.5, 25, 37.5, 50, 62.5, 75, 87.5, and 100. For example:
- A patient weighs 64 kg. The dose is 10 mg per kg.
Calculated Dose: 64 kg × 10 mg per kg = 640 mg
- The closest doses evenly divisible by 12.5 mg below and above 640 mg are 637.5 mg and 650 mg.
The nearest dose to 640 mg is 637.5 mg.
- Therefore, the actual prescribed dose for the patient should be 637.5 mg.
Table 1: Dosinga,b of NULOJIX for Kidney Transplant Recipients|
a [See Clinical Studies (14.1)] | |
|
Dosing for Initial Phase |
Dose |
|
Day 1 (day of transplantation, prior to implantation) and Day 5 (approximately 96 hours after Day 1 dose) |
10 mg per kg |
|
End of Week 2 and Week 4 after transplantation |
10 mg per kg |
|
End of Week 8 and Week 12 after transplantation |
10 mg per kg |
|
Dosing for Maintenance Phase |
Dose |
|
End of Week 16 after transplantation and every 4 weeks (plus or minus 3 days) thereafter |
5 mg per kg |
2.2 Preparation and Administration Instructions
NULOJIX is for intravenous infusion only.
Caution: NULOJIX must be reconstituted/prepared using only the silicone- free disposable syringe provided with each vial.
If the silicone-free disposable syringe is dropped or becomes contaminated, use a new silicone-free disposable syringe from inventory.
Preparation for Administration
Calculate the number of NULOJIX vials required to provide the total infusion dose. Each vial contains 250 mg of belatacept lyophilized powder.
Reconstitute the contents of each vial of NULOJIX with 10.5 mL of a suitable diluent using the silicone-free disposable syringe provided with each vial and an 18- to 21-gauge needle. Suitable diluents include: sterile water for injection (SWFI), 0.9% sodium chloride (NS), or 5% dextrose in water (D5W).
Note: If the NULOJIX powder is accidentally reconstituted using a different syringe than the one provided, the solution may develop a few translucent particles. Discard any solutions prepared using siliconized syringes.
To reconstitute the NULOJIX powder, remove the flip-top from the vial and wipe the top with an alcohol swab. Insert the syringe needle into the vial through the center of the rubber stopper and direct the stream of diluent (10.5 mL of SWFI, NS, or D5W) to the glass wall of the vial.
To minimize foam formation, rotate the vial and invert with gentle swirling until the contents are completely dissolved. Avoid prolonged or vigorous agitation. Do not shake.
The reconstituted solution contains a belatacept concentration of 25 mg/mL and should be clear to slightly opalescent and colorless to pale yellow. Do not use if opaque particles, discoloration, or other foreign particles are present.
Calculate the total volume of the reconstituted 25 mg/mL NULOJIX solution required to provide the total infusion dose.
Volume of 25 mg/mL NULOJIX solution (in mL) = Prescribed Dose (in mg) ÷ 25 mg/mL
Prior to intravenous infusion, the required volume of the reconstituted NULOJIX solution must be further diluted with a suitable infusion fluid (NS or D5W). NULOJIX reconstituted with:
•
SWFI should be further diluted with either NS or D5W
•
NS should be further diluted with NS
•
D5W should be further diluted with D5W
8.
From the appropriate size infusion bag or bottle, withdraw a volume of infusion fluid that is equal to the volume of the reconstituted NULOJIX solution required to provide the prescribed dose. With the same silicone-free disposable syringe used for reconstitution, withdraw the required amount of belatacept solution from the vial, inject it into the infusion bag or bottle, and gently rotate the infusion bag or bottle to ensure mixing.
The final belatacept concentration in the infusion bag or bottle should range from 2 mg/mL to 10 mg/mL. Typically, an infusion volume of 100 mL will be appropriate for most patients and doses, but total infusion volumes ranging from 50 mL to 250 mL may be used. Any unused solution remaining in the vials must be discarded.
Prior to administration, the NULOJIX infusion should be inspected visually for particulate matter and discoloration. Discard the infusion if any particulate matter or discoloration is observed.
The entire NULOJIX infusion should be administered over a period of 30 minutes and must be administered with an infusion set and a sterile, non-pyrogenic, low-protein-binding filter (with a pore size of 0.2 to 1.2 µm).
•
The reconstituted solution should be transferred from the vial to the infusion bag or bottle immediately. The NULOJIX infusion must be completed within 24 hours of reconstitution of the NULOJIX lyophilized powder. If not used immediately, the infusion solution may be stored under refrigeration conditions: 2°C to 8°C (36°F to 46°F) and protected from light for up to 24 hours (a maximum of 4 hours of the total 24 hours can be at room temperature: 20°C to 25°C [68°F to 77°F] and room light).
•
Infuse NULOJIX in a separate line from other concomitantly infused agents. NULOJIX should not be infused concomitantly in the same intravenous line with other agents. No physical or biochemical compatibility studies have been conducted to evaluate the coadministration of NULOJIX with other agents [see Warnings and Precautions (5.9)].
•
Use of higher than recommended or more frequent dosing is not recommended due to increased risk of serious infections and malignancy. (5.1, 5.4, 6.1)
•
For complete dosing instructions, see full prescribing information. (2.1)
|
Dosing for Initial Phase |
Dose |
|
Day 1 (day of transplantation, prior to implantation) and Day 5 (approximately 96 hours after Day 1 dose) |
10 mg per kg |
|
End of Week 2 and Week 4 after transplantation |
10 mg per kg |
|
End of Week 8 and Week 12 after transplantation |
10 mg per kg |
|
Dosing for Maintenance Phase |
Dose |
|
End of Week 16 after transplantation and every 4 weeks (plus or minus 3 days) thereafter |
5 mg per kg |
•
For intravenous infusion only; administer over 30 minutes. (2.1, 2.2)
•
Only use the enclosed silicone-free disposable syringe to prepare for administration. (2.2)
DESCRIPTION SECTION
11 DESCRIPTION
NULOJIX® (belatacept), a selective T cell costimulation blocker, is a soluble fusion protein consisting of the modified extracellular domain of CTLA-4 fused to a portion (hinge-CH2-CH3 domains) of the Fc domain of a human immunoglobulin G1 antibody. Belatacept is produced by recombinant DNA technology in a mammalian cell expression system. Two amino acid substitutions (L104 to E; A29 to Y) were made in the ligand binding region of CTLA-4. As a result of these modifications, belatacept binds CD80 and CD86 more avidly than abatacept, the parent CTLA4-Immunoglobulin (CTLA4-Ig) molecule from which it is derived. The molecular weight of belatacept is approximately 90 kilodaltons.
NULOJIX is supplied as a sterile, white or off-white lyophilized powder for intravenous administration. Prior to use, the lyophile is reconstituted with a suitable fluid to obtain a clear to slightly opalescent, colorless to pale yellow solution, with a pH in the range of 7.2 to 7.8. Suitable fluids for constitution of the lyophile include SWFI, 0.9% NS, or D5W [see Dosage and Administration (2.2)]. Each 250 mg single-use vial of NULOJIX also contains: monobasic sodium phosphate (34.5 mg), sodium chloride (5.8 mg), and sucrose (500 mg).
INFORMATION FOR PATIENTS SECTION
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Post-Transplant Lymphoproliferative Disorder
The overall risk of PTLD, especially CNS PTLD, was elevated in NULOJIX-treated patients. Instruct patients to immediately report any of the following neurological, cognitive, or behavioral signs and symptoms during and after therapy with NULOJIX [see Boxed Warning and Warnings and Precautions (5.1)]:
•
changes in mood or usual behavior
•
confusion, problems thinking, loss of memory
•
changes in walking or talking
•
decreased strength or weakness on one side of the body
•
changes in vision
Other Malignancies
Inform patients about the increased risk of malignancies, in addition to PTLD, while taking immunosuppressive therapy, especially skin cancer. Instruct patients to limit exposure to sunlight and UV light by wearing protective clothing and using a sunscreen with a high protection factor. Instruct patients to look for any signs and symptoms of skin cancer, such as suspicious moles or lesions [see Warnings and Precautions (5.3)].
Progressive Multifocal Leukoencephalopathy
Cases of PML have been reported in NULOJIX-treated patients. Instruct patients to immediately report any of the following neurological, cognitive, or behavioral signs and symptoms during and after therapy with NULOJIX [see Warnings and Precautions (5.4)]:
•
changes in mood or usual behavior
•
confusion, problems thinking, loss of memory
•
changes in walking or talking
•
decreased strength or weakness on one side of the body
•
changes in vision
Other Serious Infections
Inform patients about the increased risk of infection while taking immunosuppressive therapy. Instruct patients to adhere to antimicrobial prophylaxis regimens as prescribed. Tell patients to immediately report any signs and symptoms of infection during therapy with NULOJIX [see Warnings and Precautions (5.5)].
Immunizations
Inform patients that vaccinations may be less effective while they are being treated with NULOJIX. Advise patients that live vaccines should be avoided [see Warnings and Precautions (5.8)].
Pregnant Women and Nursing Mothers
Inform patients that NULOJIX has not been studied in pregnant women or nursing mothers so the effects of NULOJIX on pregnant women or nursing infants are not known. Instruct patients to tell their healthcare provider if they are pregnant, become pregnant, or are thinking about becoming pregnant [see Use in Specific Populations (8.1)]. Instruct patients to tell their healthcare provider if they plan to breast-feed their infant [see Use in Specific Populations (8.2)].
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
14.1 Prevention of Organ Rejection in Kidney Transplant Recipients
The efficacy and safety of NULOJIX in de novo kidney transplantation were assessed in two open-label, randomized, multicenter, active-controlled trials (Study 1 and Study 2). These trials evaluated two dose regimens of NULOJIX, the recommended dosage regimen [see Dosage and Administration (2.1)] and a regimen with higher cumulative doses and more frequent dosing than the recommended dosage regimen, compared to a cyclosporine control regimen. All treatment groups also received basiliximab induction, mycophenolate mofetil (MMF), and corticosteroids.
Treatment Regimen
The NULOJIX recommended regimen consisted of a 10 mg per kg dose administered on Day 1 (the day of transplantation, prior to implantation), Day 5 (approximately 96 hours after the Day 1 dose), end of Weeks 2 and 4; then every four weeks through Week 12 after transplantation. Starting at Week 16 after transplantation, NULOJIX was administered at the maintenance dose of 5 mg per kg every four weeks (plus or minus three days). NULOJIX was administered as an intravenous infusion over 30 minutes [see Dosage and Administration (2.1)].
Basiliximab 20 mg was administered intravenously on the day of transplantation and four days later.
The initial dose of MMF was 1 gram twice daily and was adjusted as needed, based on clinical signs of adverse events or efficacy failure.
The protocol-specified dosing of corticosteroids in Studies 1 and 2 at Day 1 was methylprednisolone (as sodium succinate) 500 mg IV on arrival in the operating room, Day 2, methylprednisolone 250 mg IV, and Day 3, prednisone 100 mg orally. Actual median corticosteroid doses used with the NULOJIX recommended regimen from Week 1 through Month 6 are summarized in the table below (Table 6).
Table 6: Actual Corticosteroida Dosing in Studies 1 and 2|
Day of Dosing |
Median (Q1–Q3) Daily Dose****b,c | |
|---|---|---|
|
Study 1 |
Study 2 | |
|
a Corticosteroid = prednisone or prednisolone. | ||
|
Week 1 |
31.7 mg (26.7-50 mg) |
30 mg (26.7-50 mg) |
|
Week 2 |
25 mg (20-30 mg) |
25 mg (20-30 mg) |
|
Week 4 |
20 mg (15-20 mg) |
20 mg (15-22.5 mg) |
|
Week 6 |
15 mg (10-20 mg) |
16.7 mg (12.5-20 mg) |
|
Month 6 |
10 mg (5-10 mg) |
10 mg (5-12.5 mg) |
Study 1 enrolled recipients of living donor and standard criteria deceased donor organs and Study 2 enrolled recipients of extended criteria donor organs. Standard criteria donor organs were defined as organs from a deceased donor with anticipated cold ischemia time of <24 hours and not meeting the definition of extended criteria donor organs. Extended criteria donors were defined as deceased donors with at least one of the following: (1) donor age ≥60 years; (2) donor age ≥50 years and other donor comorbidities (≥2 of the following: stroke, hypertension, serum creatinine >1.5 mg/dL); (3) donation of organ after cardiac death; or (4) anticipated cold ischemia time of the organ of ≥24 hours. Study 1 excluded recipients undergoing a first transplant whose current Panel Reactive Antibodies (PRA) were ≥50% and recipients undergoing a retransplantation whose current PRA were ≥30%; Study 2 excluded recipients with a current PRA ≥30%. Both studies excluded recipients with HIV, hepatitis C, or evidence of current hepatitis B infection; recipients with active tuberculosis; and recipients in whom intravenous access was difficult to obtain.
Efficacy data are presented for the NULOJIX recommended regimen and cyclosporine regimen in Studies 1 and 2.
The NULOJIX regimen with higher cumulative doses and more frequent dosing of belatacept was associated with more efficacy failures. Higher doses and/or more frequent dosing of NULOJIX are not recommended [see Dosage and Administration (2.1), Warnings and Precautions (5.1), and Adverse Reactions (6.1)].
Study 1: Recipients of Living Donor and Standard Criteria Deceased Donor
Kidneys
In Study 1 (NCT00256750), 666 patients were enrolled, randomized, and transplanted: 226 to the NULOJIX recommended regimen, 219 to the NULOJIX regimen with higher cumulative doses and more frequent dosing than recommended, and 221 to cyclosporine control regimen. The median age was 45 years; 58% of organs were from living donors; 3% were re-transplanted; 69% of the study population was male; 61% of patients were white, 8% were black/African-American, 31% were categorized as of other races; 16% had PRA ≥10%; 41% had 4 to 6 HLA mismatches; and 27% had diabetes prior to transplant. The incidence of delayed graft function was similar in all treatment arms (14% to 18%).
Premature discontinuation from treatment at the end of the first year occurred in 19% of patients receiving the NULOJIX recommended regimen and 19% of patients on the cyclosporine regimen. Among the patients who received the NULOJIX recommended regimen, 10% discontinued due to lack of efficacy, 5% due to adverse events, and 4% for other reasons. Among the patients who received the cyclosporine regimen, 9% discontinued due to adverse events, 5% due to lack of efficacy, and 5% for other reasons.
At the end of three years, 25% of patients receiving the NULOJIX recommended regimen and 34% of patients receiving the cyclosporine regimen had discontinued from treatment. Among the patients who received the NULOJIX recommended regimen, 12% discontinued due to lack of efficacy, 7% due to adverse events, and 6% for other reasons. Among the patients who received the cyclosporine regimen, 15% discontinued due to adverse events, 8% due to lack of efficacy, and 11% for other reasons.
Assessment of Efficacy
Table 7 summarizes the results of Study 1 following one and three years of treatment with the NULOJIX recommended dosage regimen and the cyclosporine control regimen. Efficacy failure at one year was defined as the occurrence of biopsy proven acute rejection (BPAR), graft loss, death, or lost to follow-up. BPAR was defined as histologically confirmed acute rejection by a central pathologist on a biopsy done for any reason, whether or not accompanied by clinical signs of rejection. Patient and graft survival was also assessed separately.
Table 7: Efficacy Outcomes by Years 1 and 3 for Study 1: Recipients of Living and Standard Criteria Deceased Donor Kidneys|
Parameter |
NULOJIX |
Cyclosporine |
NULOJIX-CSA (97.3% CI) |
|---|---|---|---|
|
a Patients may have experienced more than one event. | |||
|
Efficacy Failure by Year 1 |
49 (21.7) |
37 (16.7) |
4.9 (−3.3, 13.2) |
|
Components of Efficacy Failurea | |||
|
Biopsy Proven Acute Rejection |
45 (19.9) |
23 (10.4) | |
|
Graft Loss |
5 (2.2) |
8 (3.6) | |
|
Death |
4 (1.8) |
7 (3.2) | |
|
Lost to follow-up |
0 |
1 (0.5) | |
|
Efficacy Failure by Year 3 |
58 (25.7) |
57 (25.8) |
−0.1 (−9.3, 9) |
|
Components of Efficacy Failurea | |||
|
Biopsy Proven Acute Rejection |
50 (22.1) |
31 (14) | |
|
Graft Loss |
9 (4) |
10 (4.5) | |
|
Death |
10 (4.4) |
15 (6.8) | |
|
Lost to follow-up |
2 (0.9) |
5 (2.3) | |
|
Patient and graft survivalb | |||
|
Year 1 |
218 (96.5) |
206 (93.2) |
3.2 (−1.5, 8.4) |
|
Year 3 |
206 (91.2) |
192 (86.9) |
4.3 (−2.2, 10.8) |
In Study 1, the rate of BPAR at one year and three years was higher in patients treated with the NULOJIX recommended regimen than the cyclosporine regimen. Of the patients who experienced BPAR with NULOJIX, 70% experienced BPAR by Month 3, and 84% experienced BPAR by Month 6. By three years, recurrent BPAR occurred with similar frequency across treatment groups (<3%). The component of BPAR determined by biopsy only (subclinical protocol-defined acute rejection) was 5% in both treatment groups.
Patients treated with the NULOJIX recommended regimen experienced episodes of BPAR classified as Banff grade IIb or higher (6% [14/226] at one year and 7% [15/226] at three years) more frequently compared to patients treated with the cyclosporine regimen (2% [4/221] at one year and 2% [5/221] at three years). Also, T cell-depleting therapy was used more frequently to treat episodes of BPAR in NULOJIX-treated patients (10%; 23/226) compared to cyclosporine- treated patients (2%; 5/221). At Month 12, the difference in mean calculated glomerular filtration rate (GFR) between patients with and without history of BPAR was 19 mL/min/1.73 m2 among NULOJIX-treated patients compared to 7 mL/min/1.73 m2 among cyclosporine-treated patients. By three years, 22% (11/50) of NULOJIX-treated patients with a history of BPAR experienced graft loss and/or death compared to 10% (3/31) of cyclosporine-treated patients with a history of BPAR; at that time point, 10% (5/50) of NULOJIX-treated patients experienced graft loss and 12% (6/50) of NULOJIX-treated patients had died following an episode of BPAR, whereas 7% (2/31) of cyclosporine-treated patients experienced graft loss and 7% (2/31) of cyclosporine-treated patients had died following an episode of BPAR. The overall prevalence of donor- specific antibodies was 5% and 11% for the NULOJIX recommended regimen and cyclosporine, respectively, up to 36 months post-transplant.
While the difference in GFR in patients with BPAR versus those without BPAR was greater in patients treated with NULOJIX than cyclosporine, the mean GFR following BPAR was similar in NULOJIX (49 mL/min/1.73 m2) and cyclosporine treated patients (43 mL/min/1.73 m2) at one year. The relationship between BPAR, GFR, and patient and graft survival is unclear due to the limited number of patients who experienced BPAR, differences in renal hemodynamics (and, consequently, GFR) across maintenance immunosuppression regimens, and the high rate of switching treatment regimens after BPAR.
Assessment of Efficacy in the EBV Seropositive Subpopulation
NULOJIX is recommended for use only in EBV seropositive patients [see Indications and Usage (1.2)].
In Study 1, approximately 87% of patients were EBV seropositive prior to transplant. Efficacy results in the EBV seropositive subpopulation were consistent with those in the total population studied.
By one year, the efficacy failure rate in the EBV seropositive population was 21% (42/202) in patients treated with the NULOJIX recommended regimen and 17% (31/184) in patients treated with cyclosporine (difference=4%, 97.3% CI [−4.8, 12.8]). Patient and graft survival was 98% (198/202) in NULOJIX-treated patients and 92% (170/184) in cyclosporine-treated patients (difference=5.6%, 97.3% CI [0.8, 10.4]).
By three years, efficacy failure was 25% in both treatment groups and patient and graft survival was 94% (187/202) in NULOJIX-treated patients compared with 88% (162/184) in cyclosporine-treated patients (difference=4.6%, 97.3% CI [−2.1, 11.3]).
Assessment of Glomerular Filtration Rate (GFR)
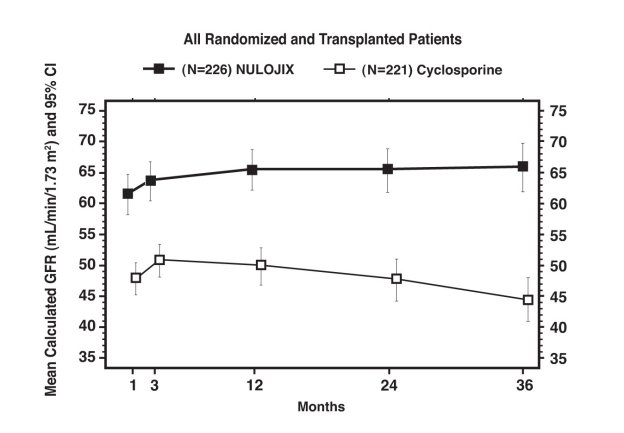
Glomerular Filtration Rate (GFR) was measured at one and two years and was calculated using the Modification of Diet in Renal Disease (MDRD) formula at one, two, and three years after transplantation. As shown in Table 8, both measured and calculated GFR was higher in patients treated with the NULOJIX recommended regimen compared to patients treated with the cyclosporine control regimen at all time points. As shown in Figure 1, the differences in GFR were apparent in the first month after transplant and were maintained up to three years (36 months). An analysis of change of calculated mean GFR between three and 36 months demonstrated an increase of 0.8 mL/min/year (95% CI [−0.2, 1.8]) for NULOJIX-treated patients and a decrease of 2.2 mL/min/year (95% CI [−3.2, −1.2]) for cyclosporine-treated patients.
Table 8: Measured and Calculated GFR for Study 1: Recipients of Living and Standard Criteria Deceased Donor Kidneys|
Parameter |
NULOJIX |
Cyclosporine |
NULOJIX-CSA (97.3% CI) |
|---|---|---|---|
|
a GFR was measured using the cold-iothalamate method. | |||
|
Measured GFRa mL/min/1.73 m2 mean (SD) | |||
|
Year 1 |
63.4 (27.7) |
50.4 (18.7) |
13.0 (7.3, 18.7) |
|
(n=206) |
(n=199) | ||
|
Year 2b |
67.9 (29.9) |
50.5 (20.5) |
17.4 (11.5, 23.4) |
|
(n=199) |
(n=185) | ||
|
Calculated GFRc mL/min/1.73 m2 mean (SD) | |||
|
Year 1 |
65.4 (22.9) |
50.1 (21.1) |
15.3 (10.3, 20.3) |
|
(n=200) |
(n=199) | ||
|
Year 2 |
65.4 (25.2) |
47.9 (23) |
17.5 (12, 23.1) |
|
(n=201) |
(n=182) | ||
|
Year 3 |
65.8 (27) |
44.4 (23.6) |
21.4 (15.4, 27.4) |
|
(n=190) |
(n=171) |
Figure 1: Calculated (MDRD) GFR Through Month 36; Study 1: Recipients of Living and Standard Criteria Deceased Donor Kidneys
Assessment of Chronic Allograft Nephropathy (CAN)
The prevalence of chronic allograft nephropathy (CAN) at one year, as defined by the Banff ’97 classification system, was 24% (54/226) in patients treated with the NULOJIX recommended regimen and in 32% (71/219) of patients treated with the cyclosporine control regimen. CAN was not evaluated after the first year following transplantation. The clinical significance of this finding is unknown.
Study 2: Recipients of Extended Criteria Donor Kidneys
In Study 2 (NCT00114777), 543 patients were enrolled, randomized, and transplanted: 175 to the NULOJIX recommended regimen, 184 to the NULOJIX regimen with higher cumulative doses and more frequent dosing than recommended, and 184 to the cyclosporine control regimen. The median age was 58 years; 67% of the study population was male; 75% of patients were white, 13% were black/African-American, 12% were categorized as of other races; 3% had PRA ≥10%; 53% had 4 to 6 HLA mismatches; and 29% had diabetes prior to transplantation. The incidence of delayed graft function was similar in all treatment arms (47% to 49%).
Premature discontinuation from treatment at the end of the first year occurred in 25% of patients receiving the NULOJIX recommended regimen and 30% of patients receiving the cyclosporine control regimen. Among the patients who received the NULOJIX recommended regimen, 14% discontinued due to adverse events, 9% due to lack of efficacy, and 2% for other reasons. Among the patients who received the cyclosporine regimen, 17% discontinued due to adverse events, 7% due to lack of efficacy, and 6% for other reasons.
At the end of three years, 35% of patients receiving the NULOJIX recommended regimen and 44% of patients receiving the cyclosporine regimen had discontinued from treatment. Among the patients who received the NULOJIX recommended regimen, 20% discontinued due to adverse events, 9% due to lack of efficacy, and 6% for other reasons. Among the patients who received the cyclosporine regimen, 25% discontinued due to adverse events, 10% due to lack of efficacy, and 10% for other reasons.
Assessment of Efficacy
Table 9 summarizes the results of Study 2 following one and three years of treatment with the NULOJIX recommended dosage regimen and the cyclosporine control regimen. Efficacy failure at one year was defined as the occurrence of biopsy proven acute rejection (BPAR), graft loss, death, or lost to follow-up. BPAR was defined as histologically confirmed acute rejection by a central pathologist on a biopsy done for any reason, whether or not accompanied by clinical signs of rejection. Patient and graft survival was also assessed.
Table 9: Efficacy Outcomes by Years 1 and 3 for Study 2: Recipients of Extended Criteria Donor Kidneys|
Parameter |
NULOJIX |
Cyclosporine |
NULOJIX-CSA (97.3% CI) |
|---|---|---|---|
|
a Patients may have experienced more than one event. | |||
|
Efficacy Failure by Year 1 |
51 (29.1) |
52 (28.3) |
0.9 (−9.7, 11.5) |
|
Components of Efficacy Failurea | |||
|
Biopsy Proven Acute Rejection |
37 (21.1) |
34 (18.5) | |
|
Graft Loss |
16 (9.1) |
20 (10.9) | |
|
Death |
5 (2.9) |
8 (4.3) | |
|
Lost to follow-up |
0 |
2 (1.1) | |
|
Efficacy Failure by Year 3 |
63 (36) |
68 (37) |
−1.0 (−12.1, 10.3) |
|
Components of Efficacy Failurea | |||
|
Biopsy Proven Acute Rejection |
42 (24) |
42 (22.8) | |
|
Graft Loss |
21 (12) |
23 (12.5) | |
|
Death |
15 (8.6) |
17 (9.2) | |
|
Lost to follow-up |
1 (0.6) |
5 (2.7) | |
|
Patient and graft survivalb | |||
|
Year 1 |
155 (88.6) |
157 (85.3) |
3.2 (−4.8, 11.3) |
|
Year 3 |
143 (81.7) |
143 (77.7) |
4.0 (−5.4, 13.4) |
In Study 2, the rate of BPAR at one year and three years was similar in patients treated with NULOJIX and cyclosporine. Of the patients who experienced BPAR with NULOJIX, 62% experienced BPAR by Month 3, and 76% experienced BPAR by Month 6. By three years, recurrent BPAR occurred with similar frequency across treatment groups (<3%). The component of BPAR determined by biopsy only (subclinical protocol-defined acute rejection) was 5% in both treatment groups.
A similar proportion of patients in the NULOJIX recommended regimen group experienced BPAR classified as Banff grade IIb or higher (5% [9/175] at one year and 6% [10/175] at three years) compared to patients treated with the cyclosporine regimen (4% [7/184] at one year and 5% [9/184] at three years). Also, T cell-depleting therapy was used with similar frequency to treat any episode of BPAR in NULOJIX-treated patients (5% or 9/175) compared to cyclosporine-treated patients (4% or 7/184). At Month 12, the difference in mean calculated GFR between patients with and without a history of BPAR was 10 mL/min/1.73 m2 among NULOJIX-treated patients compared to 14 mL/min/1.73 m2 among cyclosporine-treated patients. By three years, 24% (10/42) of NULOJIX- treated patients with a history of BPAR experienced graft loss and/or death compared to 31% (13/42) of cyclosporine-treated patients with a history of BPAR; at that time point, 17% (7/42) of NULOJIX-treated patients experienced graft loss and 14% (6/42) of NULOJIX-treated patients had died following an episode of BPAR, whereas 19% (8/42) of cyclosporine-treated patients experienced graft loss and 19% (8/42) of cyclosporine-treated patients had died following an episode of BPAR. The overall prevalence of donor-specific antibodies was 6% and 15% for the NULOJIX recommended regimen and cyclosporine, respectively, up to 36 months post-transplant.
The mean GFR following BPAR was 36 mL/min/1.73 m2 in NULOJIX patients and 24 mL/min/1.73 m2 in cyclosporine-treated patients at one year. The relationship between BPAR, GFR, and patient and graft survival is unclear due to the limited number of patients who experienced BPAR, differences in renal hemodynamics (and, consequently, GFR) across maintenance immunosuppression regimens, and the high rate of switching treatment regimens after BPAR.
Assessment of Efficacy in the EBV Seropositive Subpopulation
NULOJIX is recommended for use only in EBV seropositive patients [see Indications and Usage (1.2)].
In Study 2, approximately 91% of the patients were EBV seropositive prior to transplant. Efficacy results in the EBV seropositive subpopulation were consistent with those in the total population studied.
By one year, the efficacy failure rate in the EBV seropositive population was 29% (45/156) in patients treated with the NULOJIX recommended regimen and 28% (47/168) in patients treated with cyclosporine (difference=0.8%, 97.3% CI [−10.3, 11.9]). Patient and graft survival rate in the EBV seropositive population was 89% (139/156) in the NULOJIX-treated patients and 86% (144/168) in cyclosporine-treated patients (difference=3.4%, 97.3% CI [−4.7, 11.5]).
By three years, efficacy failure was 35% (54/156) in NULOJIX-treated patients and 36% (61/168) in cyclosporine-treated patients. Patient and graft survival was 83% (130/156) in NULOJIX-treated patients compared with 77% (130/168) in cyclosporine-treated patients (difference=5.9%, 97.3% CI [−3.8, 15.6]).
Assessment of Glomerular Filtration Rate (GFR)
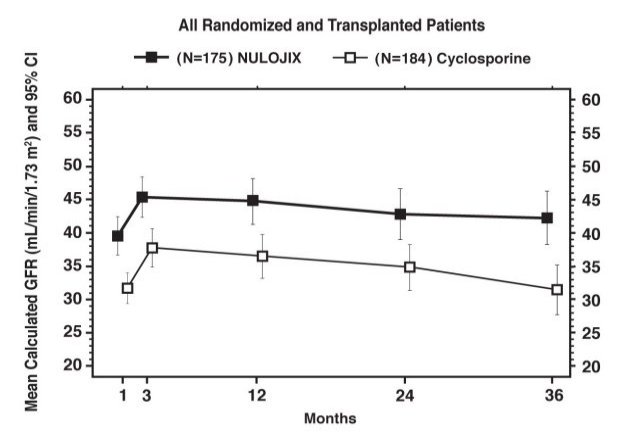
Glomerular Filtration Rate (GFR) was measured at one and two years and was calculated using the Modification of Diet in Renal Disease (MDRD) formula at one, two, and three years after transplantation. As shown in Table 10, both measured and calculated GFR was higher in patients treated with the NULOJIX recommended regimen compared to patients treated with the cyclosporine control regimen at all time points. As shown in Figure 2, the differences in GFR were apparent in the first month after transplant and were maintained up to three years (36 months). An analysis of change of calculated mean GFR between Month 3 and Month 36 demonstrated a decrease of 0.8 mL/min/year (95% CI [−1.9, 0.3]) for NULOJIX-treated patients and a decrease of 2.0 mL/min/year (95% CI [−3.1, −0.8]) for cyclosporine-treated patients.
Table 10: Measured and Calculated GFR for Study 2: Recipients of Extended Criteria Donor Kidneys|
Parameter |
NULOJIX |
Cyclosporine |
NULOJIX-CSA (97.3% CI) |
|---|---|---|---|
|
a GFR was measured using the cold-iothalamate method. | |||
|
Measured GFRa mL/min/1.73 m2 mean (SD) | |||
|
Year 1 |
49.6 (25.8) |
45.2 (21.1) |
4.3 (−1.5, 10.2) |
|
(n=151) |
(n=154) | ||
|
Year 2b |
49.7 (23.7) |
45.0 (27.2) |
4.7 (−1.8, 11.3) |
|
(n=139) |
(n=136) | ||
|
Calculated GFRc mL/min/1.73 m2 mean (SD) | |||
|
Year 1 |
44.5 (21.8) |
36.5 (21.1) |
8.0 (2.5, 13.4) |
|
(n=158) |
(n=159) | ||
|
Year 2 |
42.8 (24.1) |
34.9 (21.6) |
8.0 (1.9, 14) |
|
(n=158) |
(n=154) | ||
|
Year 3 |
42.2 (25.2) |
31.5 (22.1) |
10.7 (4.3, 17.2) |
|
(n=154) |
(n=143) |
Figure 2: Calculated (MDRD) GFR Through Month 36; Study 2: Recipients of Extended Criteria Donor Kidneys
Assessment of Chronic Allograft Nephropathy (CAN)
The prevalence of chronic allograft nephropathy (CAN) at one year, as defined by the Banff ’97 classification system, was 46% (80/174) in patients treated with the NULOJIX recommended regimen and 52% (95/184) of patients treated with the cyclosporine control regimen. CAN was not evaluated after the first year following transplantation. The clinical significance of this finding is unknown.
14.2 Long-Term Extension (LTE) of Study 1 and Study 2
Although initially designed as three-year studies, Studies 1 and 2 were subsequently extended to seven years to provide descriptive long-term safety and efficacy data. Only patients who completed the assigned treatment for three years and consented to remain on the assigned treatment from three to seven years were eligible for the long-term extension (LTE) studies.
Long-Term Extension of Study 1
In the LTE of Study 1, of the 666 originally randomized and transplanted patients, 457 (69%) patients enrolled into the LTE study: 73% (166/226) in the NULOJIX recommended regimen group, 71% (155/219) in the NULOJIX nonrecommended regimen group, and 62% (136/221) in the cyclosporine group. Fourteen (2%) patients who completed the assigned treatment at the end of Year 3 did not enroll into the LTE study: 4 in the NULOJIX recommended regimen group, 3 in the NULOJIX nonrecommended regimen group, and 7 in the cyclosporine group.
Of the 457 patients enrolled in the LTE study, 356 (79%) patients completed the assigned treatment at the end of Year 7: 82% (136/166) in the NULOJIX recommended regimen group, 83% (128/155) in the NULOJIX nonrecommended regimen group, and 68% (92/136) in the cyclosporine group. The most common reasons for discontinuation from the LTE study included adverse events and death.
Seven (4.2%) deaths and 2 (1.2%) graft losses were reported in the NULOJIX recommended regimen group while 7 (4.5%) deaths and no graft loss were reported in the NULOJIX nonrecommended regimen group, and 10 (7.4%) deaths and 6 (4.4%) graft losses were reported in the cyclosporine group.
No PTLD was reported in the NULOJIX groups while 1 case of non-CNS PTLD was reported in the cyclosporine group, in a patient who was EBV seropositive at the time of transplant.
No PML was reported in the NULOJIX groups while 1 case of PML was reported in the cyclosporine group at 82 months post-transplant (56 days after discontinuing therapy).
The higher calculated GFR observed in NULOJIX-treated patients compared to cyclosporine-treated patients during the first three years was maintained during the LTE period.
Table 11: Events Reported in Long-Term Extension from 36 to 84 Months Post-Transplant of Study 1: Recipients of Living and Standard Criteria Deceased Donor Kidneys|
NULOJIX N=166 |
NULOJIX N=155 |
Cyclosporine N=136 | |
|---|---|---|---|
|
a This patient was EBV seropositive at the time of transplant. | |||
|
Death |
7 (4.2) |
7 (4.5) |
10 (7.4) |
|
Graft Loss |
2 (1.2) |
0 (0) |
6 (4.4) |
|
Death or Graft Loss |
9 (5.4) |
7 (4.5) |
14 (10.3) |
|
PTLD |
0 (0) |
0 (0) |
1a (0.7) |
|
PML |
0 (0) |
0 (0) |
1 (0.7) |
Long-Term Extension of Study 2
In the LTE of Study 2, of the 543 originally randomized and transplanted patients, 304 (56%) patients enrolled into the LTE study: 65% (113/175) in the NULOJIX recommended regimen group, 57% (104/184) in the NULOJIX nonrecommended regimen group, and 47% (87/184) in the cyclosporine group. Nineteen (3.5%) patients who completed the assigned treatment at the end of Year 3 did not enroll into the LTE study: 1 in the NULOJIX recommended regimen group, 5 in the NULOJIX nonrecommended regimen group, and 13 in the cyclosporine group.
Of the 304 patients enrolled in the LTE study, 215 (71%) patients completed the assigned treatment at the end of Year 7: 74% (84/113) in the NULOJIX recommended regimen group, 71% (74/104) in the NULOJIX nonrecommended regimen group, and 66% (57/87) in the cyclosporine group. The most common reasons for discontinuation from the LTE study included adverse events and death.
Twenty-one (18.6%) deaths and 1 (0.9%) graft loss were reported in the NULOJIX recommended regimen group while 14 (13.5%) deaths and 2 (1.9%) graft losses were reported in the NULOJIX nonrecommended regimen group, and 9 (10.3%) deaths and 6 (6.9%) graft losses were reported in the cyclosporine group.
Six cases of PTLD were reported among the three treatment groups: 4 in the NULOJIX recommended regimen group, 1 in the NULOJIX nonrecommended regimen group, and 1 in the cyclosporine group. Three of these cases (1 in each treatment group) occurred in patients who were EBV seropositive at the time of transplant and the other 3 cases (in NULOJIX recommended regimen) occurred in patients who were EBV seronegative. No case of PML was reported among the three treatment groups.
The higher mean calculated GFR observed in NULOJIX-treated patients compared to cyclosporine-treated patients during the first three years was maintained during the LTE period.
Table 12: Events Reported in Long-Term Extension from 36 to 84 Months Post-Transplant of Study 2: Recipients of Extended Criteria Donor Kidneys|
NULOJIX N=113 |
NULOJIX N=104 |
Cyclosporine N=87 | |
|---|---|---|---|
|
a Three of these patients were EBV seronegative at the time of transplant. | |||
|
Death |
21 (18.6) |
14 (13.5) |
9 (10.3) |
|
Graft Loss |
1 (0.9) |
2 (1.9) |
6 (6.9) |
|
Death or Graft Loss |
22 (19.5) |
16 (15.4) |
14 (16.1) |
|
PTLD |
4a (3.6) |
1 (1.0) |
1 (1.2) |
|
PML |
0 (0) |
0 (0) |
0 (0) |
14.3 Follow-Up Data of Patients with Complete 7-Year Patient and Graft
Survival
In Study 1, of the original intention-to-treat (ITT) population (N=666), 72% (163/226) of patients in the NULOJIX recommended regimen group, 70% (153/219) of patients in the NULOJIX nonrecommended regimen group and 60% (132/221) of patients in the cyclosporine group had complete 7-year patient and graft survival follow-up data. Among these completers, the proportion of patients who died or had graft loss was 17% (27/163) in the NULOJIX recommended regimen group, 16% (25/153) in the NULOJIX nonrecommended regimen group and 30% (40/132) in the cyclosporine group.
In Study 2, of the original ITT population (N=543), 79% (138/175) of patients in the NULOJIX recommended regimen group, 128/184 (70%) of patients in the NULOJIX nonrecommended regimen group and 59% (108/184) of patients in the cyclosporine group had complete 7-year patient and graft survival follow-up data. Among these completers, the proportion of patients who died or had graft loss was 39% (54/138) in the NULOJIX recommended regimen group, 42% (54/128) in the NULOJIX nonrecommended regimen group and 48% (52/108) in the cyclosporine group.
Table 13: Events Reported in Patients with Complete 7-Year Patient and Graft Survival Follow-Up Data|
NULOJIX n (%) |
NULOJIX n (%) |
Cyclosporine n (%) | |
|---|---|---|---|
|
Study 1 |
N=163 |
N=153 |
N=132 |
|
** Death** |
17 (10%) |
17 (11%) |
26 (20%) |
|
** Graft Loss** |
11 (7%) |
10 (7%) |
17 (13%) |
|
** Death or Graft Loss** |
27 (17%) |
25 (16%) |
40 (30%) |
|
Study 2 |
N=138 |
N=128 |
N=108 |
|
** Death** |
37 (27%) |
37 (29%) |
29 (27%) |
|
** Graft Loss** |
23 (17%) |
21 (16%) |
29 (27%) |
|
** Death or Graft Loss** |
54 (39%) |
54 (42%) |
52 (48%) |