
ONAPGO
ONAPGO - These highlights do not include all the information needed to use ONAPGO safely and effectively. See full prescribing information for ONAPGO. ONAPGO (apomorphine hydrochloride) injection, for subcutaneous use Initial U.S. Approval: 2004
f3552b6e-5ae7-4993-aa1a-e399c4a7080a
HUMAN PRESCRIPTION DRUG LABEL
Jul 7, 2025
MDD US Operations, LLC, a subsidiary of Supernus Pharmaceuticals, Inc
DUNS: 087875626
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Apomorphine hydrochloride
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (4)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
PRINCIPAL DISPLAY PANEL - 20 mL Cartridge Carton
ONAPGO™
(apomorphine HCl)
injection, for subcutaneous use
NDC 27505-006-05
Rx Only
98 mg/20 mL (4.9 mg/mL)
Single-dose cartridge.
Discard unused portion.
Package contains 5 x 20 mL cartridges
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
ONAPGO is indicated for the treatment of motor fluctuations in adults with advanced Parkinson's disease.
ONAPGO is a dopaminergic agonist indicated for the treatment of motor fluctuations in adults with advanced Parkinson's disease. ( 1)
CONTRAINDICATIONS SECTION
4 CONTRAINDICATIONS
ONAPGO is contraindicated in patients:
- Using concomitant 5HT 3antagonists, including antiemetics (e.g., ondansetron, granisetron, dolasetron, palonosetron) and alosetron [see Drug Interactions (7.1)] . There have been reports of profound hypotension and loss of consciousness when apomorphine was administered with ondansetron.
- With hypersensitivity/allergic reaction to apomorphine or any of the excipients of ONAPGO, including sulfite (i.e., sodium metabisulfite). Angioedema or anaphylaxis may occur [see Warnings and Precautions (5.13)].
- Concomitant use of ONAPGO with 5HT 3antagonists, including antiemetics (e.g., ondansetron, granisetron, dolasetron, palonosetron) and alosetron. ( 4, 7.1)
- Hypersensitivity to apomorphine or the excipients of ONAPGO, including sulfite (i.e., sodium metabisulfite). ( 4, 5.13)
WARNINGS AND PRECAUTIONS SECTION
5 WARNINGS AND PRECAUTIONS
5.1 Serious Adverse Reactions After Intravenous Administration
Following intravenous administration of apomorphine, serious adverse reactions including thrombus formation and pulmonary embolism caused by intravenous crystallization of apomorphine have occurred. Do not administer ONAPGO intravenously.
5.2 Nausea and Vomiting
ONAPGO is known to cause nausea and vomiting, which may be severe. In Study 1 [see Clinical Studies (14)] 87% of patients were pretreated with an antiemetic. Twenty-two percent of patients treated with ONAPGO reported nausea and 7% reported vomiting, compared to 9% and 4%, respectively, of patients who received placebo. The ability of concomitantly administered antiemetic drugs (other than trimethobenzamide) to reduce apomorphine-associated nausea/vomiting has not been studied. Antiemetics with anti-dopaminergic actions (e.g., haloperidol, chlorpromazine, promethazine, prochlorperazine, metoclopramide) have the potential to worsen the symptoms in patients with PD and therefore the benefits and risks of treatment with these antiemetics should be carefully considered. The use of ONAPGO with 5HT 3antiemetics is contraindicated.
5.3 Falling Asleep During Activities of Daily Living and Somnolence
Somnolence is commonly associated with ONAPGO**.**Patients treated with dopaminergic medications, including apomorphine, have also reported falling asleep while engaged in activities of daily living, including the operation of motor vehicles, which sometimes resulted in accidents. Patients may not perceive warning signs, such as excessive drowsiness, or they may report feeling alert immediately prior to the event. In the double-blind placebo- controlled trial (Study 1), somnolence was reported in 22% of patients treated with ONAPGO and 4% of patients in the placebo group.
Falling asleep while engaged in activities of daily living usually occurs in patients experiencing preexisting somnolence, although patients may not give such a history. Therefore, prescribers should reassess patients for drowsiness or sleepiness while using ONAPGO, especially because some of the events occur well after the start of treatment. Prescribers should also be aware that patients may not acknowledge drowsiness or sleepiness until directly questioned about drowsiness or sleepiness during specific activities.
Before initiating treatment with ONAPGO, advise patients of the risk of drowsiness and ask them about factors that could increase the risk with ONAPGO, such as concomitant sedating medications and the presence of sleep disorders. If a patient develops significant daytime sleepiness or falls asleep during activities that require active participation (e.g., conversations, eating, etc.), ONAPGO should ordinarily be discontinued. If a decision is made to continue ONAPGO, patients should be advised not to drive and to avoid other potentially dangerous activities. There is insufficient information to determine whether dose reduction will eliminate episodes of falling asleep while engaged in activities of daily living.
5.4 Syncope/Hypotension/Orthostatic Hypotension
Dopamine agonists, including ONAPGO, may cause orthostatic hypotension at any time, but especially during dose escalation. Patients with PD may also have an impaired capacity to respond to an orthostatic challenge. For these reasons, PD patients being treated with dopaminergic agonists should be monitored for signs and symptoms of orthostatic hypotension, especially during dose escalation, and should be informed of this risk.
When evaluated at various times after dosing in Study 1, patients undergoing titration of ONAPGO showed an increased incidence (from 4.5% pre-dose to 44.4% post-dose) of systolic orthostatic hypotension (≥ 20 mm Hg decrease upon standing) compared to placebo (7.1% pre-dose to 16.3% post-dose). Similarly, increased incidences of diastolic orthostatic hypotension (≥ 10 mm Hg decrease upon standing) were noted in patients titrated with ONAPGO (4.5% pre-dose to 44.4% post-dose) compared to placebo (11.9% pre-dose to 30.2% post-dose). Through the 12-week treatment period, these differences in incidence rates for systolic and diastolic orthostatic hypotension remained similar between ONAPGO and placebo patients. Patients in both ONAPGO and placebo groups developed severe systolic orthostatic hypotension (≥ 40 mm Hg decrease) and/or diastolic orthostatic hypotension (≥ 20 mm Hg decrease).
In Study 1, 13% of patients treated with ONAPGO reported hypotension or orthostatic hypotension compared to 2% of patients who received placebo [hypotension (7% vs 0%), orthostatic hypotension (4% vs 2%), and orthostatic intolerance (2% vs 0%)]. In the double-blind period of Study 1, one patient (2%) experienced a serious adverse event of hypotension and withdrew from the study compared to none in placebo.
Syncope has been reported in patients who have received subcutaneous apomorphine.
Patients with PD may also have an impaired capacity to respond to an orthostatic challenge. For these reasons, PD patients being treated with dopaminergic agonists ordinarily require careful monitoring for signs and symptoms of orthostatic hypotension, especially during dose escalation, and should be informed of this risk. Patients should avoid alcohol when using ONAPGO [see Drug Interactions (7.3)] . Patients taking ONAPGO should lie down before and after taking sublingual nitroglycerin. Other vasodilators and antihypertensives may also increase the hypotensive effects of ONAPGO. Monitor blood pressure for hypotension and orthostatic hypotension in patients taking ONAPGO with concomitant antihypertensive medications or vasodilators [see Drug Interactions (7.2)].
5.5 Falls
Patients with Parkinson's disease are at risk of falling due to underlying postural instability, possible autonomic instability, and syncope caused by the blood pressure lowering effects of the drugs used to treat Parkinson's disease. ONAPGO might increase the risk of falling by simultaneously lowering blood pressure and altering mobility [see Warnings and Precautions (5.4)and Clinical Pharmacology (12.2)]. Falls, including serious falls, have been reported in patients treated with apomorphine.
5.6 Infusion Site Reactions and Infections
ONAPGO can cause infusion site reactions and infections.
In Study 1, one or more infusion site reactions were reported in 63% of patients treated with ONAPGO and 15% in patients who received placebo. Various types of reactions at the infusion site have been reported including nodules, erythema, hematomas, inflammation, pruritus, swelling, discoloration, hemorrhage, hypersensitivity, induration, edema, pain, rash, or bruising [see Adverse Reactions (6.1)] . In Study 1, 2% of patients treated with ONAPGO and no patient who received placebo discontinued treatment because of an infusion site reaction.
Infusion site infections occurred in 4% of patients treated with ONAPGO compared to no patients who received placebo. The most frequent infusion site infection reported was cellulitis. If an infection is suspected at the infusion site, the cannula should be removed from the infusion site. If the cannula is removed for an infection, a new cannula should be placed at a new infusion site. In the event of a prolonged interruption of treatment with ONAPGO, the patient should be prescribed oral medications to treat their Parkinson's disease [see Dosage and Administration (2.4)].
5.7 Hallucinations/Psychotic-Like Behavior
In Study 1, 4% of patients treated with ONAPGO reported hallucinations compared to 4% of patients who received placebo. Psychotic disorder was reported in 2% of patients treated with ONAPGO compared to none who received placebo.
Postmarketing reports with intermittent subcutaneous apomorphine indicate that patients may experience new or worsening mental status and behavioral changes, which may be severe, including psychotic-like behavior after starting or increasing the dose of apomorphine. Other drugs prescribed to improve the symptoms of PD can have similar effects on thinking and behavior. This abnormal thinking and behavior can consist of one or more of a variety of manifestations, including paranoid ideation, delusions, hallucinations, confusion, disorientation, aggressive behavior, agitation, and delirium. Consider the risks and benefits prior to initiating treatment with ONAPGO in patients with a major psychotic disorder because of the risk of exacerbating psychosis. In addition, certain medications used to treat psychosis may exacerbate the symptoms of PD and may decrease the effectiveness of ONAPGO [see Drug Interactions (7.3)] .
5.8 Dyskinesia
ONAPGO may cause dyskinesia or exacerbate pre-existing dyskinesia. In Study 1, dyskinesia or worsening of dyskinesia was reported in approximately 15% of patients treated with ONAPGO compared to no patients who received placebo.
5.9 Hemolytic Anemia
Hemolytic anemia requiring hospitalization has been reported with apomorphine treatment in a postmarketing setting. Many of the reported cases included positive direct antiglobulin test (Coombs test), suggesting a potential immune-mediated hemolysis. Severe anemia, angina, and dyspnea have occurred with hemolytic anemia. Some patients were treated with high dose glucocorticoids or blood transfusions. Hemolytic anemia can occur at any time after apomorphine treatment. If a patient develops anemia while taking ONAPGO, consider a workup for hemolytic anemia. If hemolytic anemia occurs, consider discontinuing treatment with ONAPGO. In Study 1, hemolytic anemia was reported in 2% of patients treated with ONAPGO compared to no patient who received placebo.
5.10 Impulse Control/Compulsive Behaviors
Patients may experience intense urges to gamble, increased sexual urges, intense urges to spend money uncontrollably, and other intense urges and the inability to control these urges while taking one or more of the medications, including ONAPGO, that increase central dopaminergic tone and that are generally used for the treatment of PD. In some cases, although not all, these urges were reported to have stopped when the dose was reduced, or the medication was discontinued. Because patients may not recognize these behaviors as abnormal, it is important for prescribers to specifically ask patients or their caregivers about the development of new or increased gambling urges, sexual urges, uncontrolled spending, or other urges while being treated with ONAPGO. Physicians should consider dose reduction or stopping the medication if a patient develops such urges while taking ONAPGO
5.11 Cardiac Events
In Study 1, 4 patients treated with ONAPGO experienced cardiac disorders, including left bundle branch block (2%), myocardial infarction (2%), palpitations (2%), or tachycardia (2%), compared to no patients who received placebo. In patients treated with apomorphine subcutaneous injection, cardiac arrest and/or sudden death has occurred; some cases of angina and myocardial infarction occurred in close proximity to apomorphine dosing (within 2 hours), while other cases of cardiac arrest and sudden death were observed at times unrelated to dosing.
ONAPGO has been shown to reduce resting systolic and diastolic blood pressure and may have the potential to exacerbate cardiac (and cerebral) ischemia in patients with known cardiovascular and cerebrovascular disease. If patients develop signs and symptoms of cardiac or cerebral ischemia, prescribers should re-evaluate the continued use of ONAPGO.
5.12 QTc Prolongation and Potential for Proarrhythmic Effects
There is a dose-related prolongation of QTc interval after apomorphine exposure similar to that achieved with therapeutic doses of ONAPGO [see Clinical Pharmacology (12.2)] . In Study 1, 4% of patients treated with ONAPGO experienced prolonged QTc interval compared to none who received placebo.
Drugs that prolong the QTc interval have been associated with torsades de pointes and sudden death. The relationship of QTc prolongation to torsades de pointes is clearest for larger increases (20 msec and greater), but it is possible that smaller QTc prolongations may also increase risk, or increase it in susceptible individuals, such as those with hypokalemia, hypomagnesemia, bradycardia, concomitant use of other drugs that prolong the QTc interval, or genetic predisposition (e.g., congenital prolongation of the QT interval). Although torsades de pointes has not been observed in association with the use of ONAPGO at recommended doses in clinical studies, experience is too limited to rule out an increased risk. Palpitations and syncope may signal the occurrence of an episode of torsades de pointes.
The risks and benefits of ONAPGO treatment should be considered prior to initiating treatment with ONAPGO in patients with risk factors for prolonged QTc.
5.13 Hypersensitivity
In Study 1, 11% of patients treated with ONAPGO reported rash (4%), infusion site pruritus (4%), infusion site rash (2%), hypersensitivity (2%), or infusion site hypersensitivity (2%) compared to no patient who received placebo. Hypersensitivity/allergic reactions characterized by urticaria, rash, pruritus, and/or various manifestations of angioedema may occur because of ONAPGO or because of its sulfite excipient. ONAPGO contains sodium metabisulfite, a sulfite that may cause allergic-type reactions, including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in certain susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown and probably low. Sulfite sensitivity is seen more frequently in asthmatic than in nonasthmatic people.
5.14 Fibrotic Complications
Cases of retroperitoneal fibrosis, pulmonary infiltrates, pleural effusion, pleural thickening, and cardiac valvulopathy have been reported in some patients treated with ergot-derived dopaminergic agents. While these complications may resolve when the drug is discontinued, complete resolution does not always occur. Although these adverse reactions are believed to be related to the ergoline structure of these dopamine agonists, whether other, non-ergot-derived dopamine agonists, such as ONAPGO, can cause these reactions is unknown.
5.15 Priapism
In clinical studies of intermittent apomorphine injection, painful erections were reported in 3 of 361 men treated with subcutaneous injection, and one patient withdrew from therapy because of priapism. Although no patients in the clinical studies required surgical intervention, severe priapism may require surgical intervention.
5.16 Retinal Pathology in Albino Rats
In a two-year carcinogenicity study of apomorphine in albino rat, retinal atrophy was detected at all subcutaneous doses tested (up to 0.8 mg/kg/day or 2 mg/kg/day in males or females, respectively; less than the maximum recommended human dose (MRHD) of 98 mg/day on a body surface area [mg/m 2] basis). Retinal atrophy/degeneration has been observed in albino rats treated with other dopamine agonists for prolonged periods (generally during two-year carcinogenicity studies). Retinal findings were not observed in a 39-week subcutaneous toxicity study of apomorphine in monkey at doses up to 1.5 mg/kg/day, a dose similar to the MRHD on a mg/m 2basis. The clinical significance of the finding in rat has not been established but cannot be disregarded because disruption of a mechanism that is universally present in vertebrates (e.g., disk shedding) may be involved.
- Subcutaneous use only; thrombus formation and pulmonary embolism have followed intravenous administration of ONAPGO. ( 5.1)
- May cause nausea and vomiting. ( 2.2, 5.2)
- Falling asleep during activities of daily living and daytime somnolence may occur. ( 5.3)
- May cause hypotension/orthostatic hypotension and syncope may occur. ( 5.4)
- May cause or increase the risk of falls. ( 5.5)
- May cause infusion site reactions and infections. Monitor and change infusion site every day. ( 2.4, 5.6)
- May cause hallucinations and psychotic-like behavior. ( 5.7)
- May cause dyskinesia or exacerbate pre-existing dyskinesia. ( 5.8)
- May cause hemolytic anemia. ( 5.9)
- May cause impulse control/ compulsive and impulsive behaviors. Consider dose reductions or stopping ONAPGO. ( 5.10)
- May cause cardiac events. ( 5.11)
- May prolong QTc and cause torsades de pointes or sudden death. ( 5.12)
ADVERSE REACTIONS SECTION
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Serious Adverse Reactions After Intravenous Administration [see Warnings and Precautions (5.1)]
- Nausea and Vomiting [see Warnings and Precautions (5.2)]
- Falling Asleep During Activities of Daily Living and Somnolence [see Warnings and Precautions (5.3)]
- Syncope/Hypotension/Orthostatic Hypotension [see Warnings and Precautions (5.4)]
- Falls [see Warnings and Precautions (5.5)]
- Infusion Site Reactions and Infections [see Warnings and Precautions (5.6)]
- Hallucinations/Psychotic-Like Behavior [see Warnings and Precautions (5.7)]
- Dyskinesia [see Warnings and Precautions (5.8)]
- Hemolytic Anemia [see Warnings and Precautions (5.9)]
- Impulse Control/Compulsive Behaviors [see Warnings and Precautions (5.10)]
- Cardiac Events [see Warnings and Precautions (5.11)]
- QTc Prolongation and Potential for Proarrhythmic Effects [see Warnings and Precautions (5.12)]
- Hypersensitivity [see Warnings and Precautions (5.13)]
- Fibrotic Complications [see Warnings and Precautions (5.14)]
- Priapism [see Warnings and Precautions (5.15)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. A total of 197 Parkinson's disease patients were exposed to ONAPGO in Study 1 and subsequent open-label studies.
In Study 1 [see Clinical Studies (14)], the most common adverse reactions (incidence 10% or greater in patients treated with ONAPGO and at a rate at least twice the placebo rate) were infusion site nodule, nausea, somnolence, infusion site erythema, dyskinesia, headache, and insomnia.
Table 1 presents adverse reactions that occurred in ≥5% of patients treated with ONAPGO and that occurred more frequently than placebo in patients who were enrolled in Study 1.
Table 1: Adverse Reactions Reported by ≥5% of Patients Treated with ONAPGO and More Frequently than Placebo in Study 1|
ONAPGO * |
Placebo | |
|---|---|---|
| ||
|
Infusion site nodule |
44 |
0 |
|
Nausea |
22 |
9 |
|
Somnolence |
22 |
4 |
|
Infusion site erythema |
17 |
4 |
|
Dyskinesia |
15 |
0 |
|
Headache |
13 |
4 |
|
Insomnia |
11 |
2 |
|
Dizziness |
9 |
4 |
|
Hypotension |
7 |
0 |
|
Asthenia |
7 |
0 |
|
Fatigue |
7 |
2 |
|
Constipation |
7 |
6 |
|
Vomiting |
7 |
4 |
Infusion Site Reactions
In Study 1, infusion site reactions were most commonly reported as nodule formation (44% of patients treated with ONAPGO compared to no patients who received placebo) or erythema (17% of patients treated with ONAPGO compared to 4% of patients who received placebo).
Less Common Adverse Reactions
Other adverse reactions, including hallucinations, psychotic disorder, impulse control disorder, prolonged QT interval, and infusion site infections [see Warnings and Precautions (5.6)] , have been reported in patients treated with ONAPGO [see Warnings and Precautions (5.7, 5.10. 5.12)].
Adverse Reactions Leading to Discontinuation of ONAPGO Treatment
Six (11%) of patients treated with ONAPGO reported one of the following adverse reactions as the reason for discontinuing from Study 1: nausea, orthostatic intolerance, visual hallucination, gait disturbance, infusion site nodule, and hypotension. None of the patients who received placebo discontinued from Study 1 because of an adverse reaction.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of apomorphine. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Hematologic and Lymphatic Systems: hemolytic anemia [see Warnings and Precautions (5.9)]
Most common adverse reactions (incidence ≥10% on ONAPGO and at least twice the rate of placebo) were infusion site nodule, nausea, somnolence, infusion site erythema, dyskinesia, headache, and insomnia. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact MDD US Operations, LLC, a subsidiary of Supernus Pharmaceuticals, Inc. at toll-free number 1-833-366-2746 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
7.1 5HT 3Antagonists
Based on reports of profound hypotension and loss of consciousness when apomorphine was administered with ondansetron, the concomitant use of ONAPGO with 5HT 3antagonists, including antiemetics (e.g., ondansetron, granisetron, palonosetron) and alosetron, is contraindicated [see Warnings and Precautions (5.4)].
7.2 Antihypertensive Medications and Vasodilators
In clinical studies with intermittent subcutaneous administration of apomorphine, the following adverse reactions were experienced more commonly in patients receiving concomitant antihypertensive medications or vasodilators (n=94) than in patients not receiving these medications (n=456): hypotension (10% vs 4%) myocardial infarction (3% vs 1%), [see Warnings and Precautions (5.4, 5.11)].
In a study of healthy subjects, concomitant administration of 0.4 mg sublingual nitroglycerin with subcutaneous apomorphine caused greater decreases in blood pressure than with subcutaneous apomorphine alone [see Clinical Pharmacology (12.3)]. Patients treated with ONAPGO should lie down before and after taking sublingual nitroglycerin to decrease the potential risks associated with hypotension .
7.3 Alcohol
In a study of healthy subjects, concomitant administration of high dose (0.6 g/kg) or low dose (0.3 g/kg) ethanol with apomorphine caused greater decreases in blood pressure than with apomorphine alone [see Clinical Pharmacology (12.3)] . Patients should be advised not to consume alcohol while treated with ONAPGO because it may cause greater decreases in blood pressure [see Warnings and Precautions (5.4)] .
7.4 Dopamine Antagonists
Because ONAPGO is a dopamine agonist, it is possible that concomitant use of dopamine antagonists, such as the neuroleptics (phenothiazines, butyrophenones, thioxanthenes) or metoclopramide, may diminish the effectiveness of ONAPGO. Antiemetics with anti-dopaminergic actions should be avoided [see Warnings and Precautions (5.2)]. Patients with major psychotic disorders, treated with neuroleptics, should be treated with dopamine agonists only if the potential benefits outweigh the risks [see Warnings and Precautions (5.7)].
7.5 Drugs Prolonging the QT/QTc Interval
Caution should be exercised when prescribing ONAPGO concomitantly with drugs that prolong the QT/QTc interval [see Warnings and Precautions (5.12)and Clinical Pharmacology (12.2)] .
- Concomitant use of antihypertensive medications and vasodilators: increased risk for hypotension, falls, and injuries. ( 7.2)
- Dopamine antagonists such as neuroleptics or metoclopramide, may diminish the effectiveness of ONAPGO. ( 7.4)
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Important Information
- ONAPGO is indicated for subcutaneous use by infusion only [see Warnings & Precautions (5.1)] .
- Patients selected for treatment with ONAPGO should be capable of understanding and trained on using the delivery system, either themselves or with the assistance of a caregiver [see Healthcare Provider Instructions for Use and Patient Instructions for Use].
- ONAPGO initiation and dose titrations should be done under medical supervision.
- The prescribed dose of ONAPGO should be expressed in "mg/hr" for the continuous dosage and "mg" for an extra dose.
2.2 Premedication and Concomitant Medication
Because of the incidence of nausea and vomiting with ONAPGO, it is recommended that treatment with trimethobenzamide 300 mg three times a day start 3 days prior to the initial dose of ONAPGO [see Adverse Reactions (6.1)and Warnings and Precautions (5.2)] . Alternatively, consider starting ONAPGO therapy, without antiemetics, at 1 mg/hour and titrate based upon effectiveness and tolerance.
If trimethobenzamide is used, it should be continued only as long as necessary to control nausea and vomiting, and generally no longer than two months after initiation of treatment with ONAPGO, as trimethobenzamide increases the incidence of somnolence, dizziness, and falls in patients treated with ONAPGO [see Warnings and Precautions (5.2)] .
Based on reports of profound hypotension and loss of consciousness when apomorphine was administered with ondansetron, the concomitant use of apomorphine with drugs of the 5HT 3antagonist class including antiemetics (e.g., ondansetron, granisetron, dolasetron, palonosetron) and alosetron are contraindicated [see Contraindications (4)] .
After starting ONAPGO, adjustment of concomitant anti-Parkinson's disease medications may be necessary.
2.3 Recommended Dosage
ONAPGO (apomorphine hydrochloride) is administered as a subcutaneous infusion with the ONAPGO pump [see Dosage and Administration (2.3), Healthcare Provider Instructions for Use, and Patient Instructions for Use].
The daily dosage is determined by individualized patient titration and is composed of a continuous dosage and as needed extra dose(s).
The maximum recommended total daily dosage of ONAPGO, including the continuous dosage and any extra dose(s), is 98 mg per day, generally administered over the waking day (e.g., 16 hours).
Continuous Dosage
The recommended initial continuous dosage (continuous infusion) of ONAPGO is 1 mg/hr. Titrate the continuous dosage, as needed, in 0.5 mg/hr to 1 mg/hr increments. Dose adjustments may be made daily, or at longer intervals, through the titration process. Patients in clinical studies used a mean of 4 mg/hr of ONAPGO. The maximum continuous dosage is 6 mg/hour administered over the waking day (e.g., 16 hours).
Extra Dose
Extra doses of ONAPGO may be used:
- upon starting in the morning; or
- when restarting the continuous dosage after a 1-hour or longer break in use (i.e., as a loading dose); or
- as a supplement to the continuous dosage to manage acute OFF symptoms that are not controlled
The extra dose may be titrated to clinical response and tolerability with adjustments in increments of 0.5 mg or 1 mg. Subsequent extra doses may be between 0.5 mg and 2 mg.
Administer no more than 3 extra doses per day over 16 hours with at least 3 hours between extra doses.
If 3 extra doses are routinely required during daily infusion, consider further adjustment of the continuous dosage.
The maximum recommended total daily dosage, including extra doses, is 98 mg during the waking day (e.g., 16 hours).
Other Apomorphine Medications
ONAPGO is not substitutable for apomorphine products intended for intermittent use. There is insufficient information about concomitant use of other apomorphine containing products with ONAPGO.
2.4 Preparation and Administration Instructions
Patients and caregivers should receive education and be trained on the proper use of ONAPGO and the device delivery system prior to first use [see Dosage and Administration (2.2)and Patient Instructions for Use].
- Visually inspect solution for particulate matter and discoloration prior to administration. Solution should be clear, almost colorless. Do not use if solution is discolored or contains particles.
- Keep the infusion site clean and use aseptic technique.
- Administer ONAPGO subcutaneously in one of the following areas:
- Abdomen at least 2 inches away from the navel
- Top of thigh
- Lower back
- Upper back, only when the infusion site is being prepared by a caregiver or healthcare provider
- Change the infusion site every day *Do notselect an infusion site that is bruised, has bumps or nodules, or is irritated.
- A new single-dose cartridge and cartridge holder should be used each day. Discard unused portion.
2.5 Recommended Dosage in Patients with Renal Impairment
For patients with mild or moderate renal impairment, the recommended initial extra dose is 0.5 mg to 1 mg and should not exceed 1 mg [see Clinical Pharmacology (12.3)and Use in Specific Populations (8.6)]. No adjustment is needed for the continuous dose, maximum recommended daily dose, or subsequent extra doses after the initial extra dose [see Dosage and Administration (2.3)]. Patients with severe renal impairment have not been studied.
2.6 Discontinuation of ONAPGO
Sudden discontinuation or rapid dose reduction of ONAPGO could result in increased severity of Parkinson's disease motor symptoms. If possible, ONAPGO should be tapered before discontinuing.
- For subcutaneous use by infusion only. ( 2.1)
- Maximum recommended total daily dosage of ONAPGO, including the continuous dosage and any extra dose(s), is 98 mg generally administered over the waking day (e.g., 16 hours). ( 2.3)
- The recommended initial continuous dosage is 1 mg/hr with a maximum of 6 mg/hr for up to 16 hours per day. ( 2.3)
- The extra dose may be titrated in increments of 0.5 mg or 1 mg based on clinical response and tolerability. Subsequent extra doses are between 0.5 mg and 2 mg, with at least 3 hours between extra doses and a maximum of 3 extra doses per day. ( 2.3)
- Treatment with trimethobenzamide is recommended, starting 3 days prior to the first dose of ONAPGO, and should only be continued as long as necessary to control nausea and vomiting, and generally no longer than two months. ( 2.2, 5.2, 6.1, 17)
- ONAPGO is not substitutable for apomorphine products intended for intermittent use. ( 2.3)
- For patients with mild or moderate renal impairment, the recommended initial extra dose is 0.5 mg to 1 mg and should not exceed 1 mg. ( 2.5)
DOSAGE FORMS & STRENGTHS SECTION
3 DOSAGE FORMS AND STRENGTHS
Injection: 98 mg/20 mL (4.9 mg/mL) apomorphine hydrochloride is a clear, almost colorless solution available in a single-dose prefilled cartridge.
Injection: 98 mg/20 mL (4.9 mg/mL) of apomorphine hydrochloride in single-dose cartridges. ( 3)
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no adequate data on the developmental risk associated with use of ONAPGO in pregnant women. In animal reproduction studies, apomorphine had adverse developmental effects in rats (increased neonatal deaths) and rabbits (increased incidence of malformation) when administered during pregnancy at clinically relevant doses. These doses were also associated with maternal toxicity. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively. The background risk of major birth defects and miscarriage for the indicated population is unknown.
Data
Animal Data
No adverse developmental effects were observed when apomorphine (0.3, 1, or 3 mg/kg/day) was administered by subcutaneous injection to pregnant rats throughout organogenesis; the highest dose tested is less than the maximum recommended human dose (MRRD) of 98 mg on a mg/m 2basis. Administration of apomorphine (0.3, 1, or 3 mg/kg/day) by subcutaneous injection to pregnant rabbits throughout organogenesis resulted in an increased incidence of malformations of the heart and/or great vessels at the mid and high doses; maternal toxicity was observed at the highest dose tested. The no-effect dose (0.3mg/kg/day) for adverse effects is less than the MRHD on a mg/m 2basis.
Apomorphine (0.3, 1, or 3 mg/kg/day), administered by subcutaneous injection to female rats throughout gestation and lactation, resulted in increased offspring mortality at the highest dose tested, which was associated with maternal toxicity. There were no effects on developmental parameters or reproductive performance in surviving offspring. The no-effect dose (1 mg/kg/day) for developmental toxicity is less than the MRHD on a mg/m 2basis.
8.2 Lactation
Risk Summary
There are no data on the presence of apomorphine in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for ONAPGO and any potential adverse effects on the breastfed infant from ONAPGO or from the underlying maternal condition.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of comorbid disease or other drug therapy.
Clinical studies of ONAPGO did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger subjects. Clinical experience with intermittent subcutaneous use of apomorphine has shown that the following adverse reactions were reported more frequently in patients 65 years of age or older (n=311) compared to patients less than 65 years of age (n=239): confusion; hallucinations; serious adverse reactions (life-threatening events or events resulting in hospitalization and/or increased disability); falls (experiencing bone and joint injuries); cardiovascular events; respiratory disorders; gastrointestinal events; and discontinuation of treatment as a result of one or more adverse reactions.
8.6 Renal Impairment
The initial extra dose of ONAPGO should not exceed 1 mg in patients with mild or moderate renal impairment because of increased apomorphine concentration and exposure (C maxand AUC) in these patients. Studies in patients with severe renal impairment have not been conducted [see Dosage and Administration (2.5)and Clinical Pharmacology (12.3)].
8.7 Hepatic Impairment
Exercise caution and closely monitor if ONAPGO is administered to patients with mild or moderate hepatic impairment because of increased apomorphine concentration and exposure (C maxand AUC) in these patients. Studies in patients with severe hepatic impairment have not been conducted [see Clinical Pharmacology (12.3)] .
- Pregnancy: Based on animal data, may cause fetal harm. ( 8.1)
DRUG ABUSE AND DEPENDENCE SECTION
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
ONAPGO contains apomorphine, which is not a controlled substance.
9.2 Abuse
In premarketing clinical experience, apomorphine did not reveal any tendency for a withdrawal syndrome or any drug-seeking behavior. However, there are rare postmarketing reports of abuse of medications containing apomorphine. In general, these reports consist of patients taking increasing doses of medication in order to achieve a euphoric state. Abuse is the intentional, non-therapeutic use of a drug, even once, for its desirable psychological or physiological effects.
DESCRIPTION SECTION
11 DESCRIPTION
ONAPGO (apomorphine hydrochloride) contains apomorphine hydrochloride hemihydrate, a non-ergoline dopamine agonist. It is chemically designated as 6aβ-aporphine-10,11-diol hydrochloride hemihydrate with a molecular formula of C 17H 17NO 2∙HCl∙½H 2O. Its structural formula and molecular weight are:

Apomorphine hydrochloride hemihydrate appears as minute, white or grayish- white glistening crystals or as white powder that is soluble in water at 80°C. ONAPGO injection is a clear, almost colorless, sterile solution for subcutaneous infusion and is available in 98 mg/20 mL (4.9 mg/mL) single-dose prefilled cartridges. The solution has a pH of 3.0 -4.0. Each mL contains 4.9 mg of apomorphine hydrochloride (equivalent to 4.27 mg apomorphine) and 0.5 mg of sodium metabisulfite in water for injection. In addition, each mL may contain hydrochloric acid used to adjust the pH.
CLINICAL PHARMACOLOGY SECTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
ONAPGO is a non-ergoline dopamine agonist with high in vitro binding affinity for the dopamine D4 receptor, and moderate affinity for the dopamine D2, D3, and D5, and adrenergic α1D, α2B, α2C receptors. The precise mechanism of action of ONAPGO as a treatment for Parkinson's disease is unknown, although it is believed to be due to stimulation of post-synaptic dopamine D2-type receptors within the caudate-putamen in the brain.
12.2 Pharmacodynamics
Prolongation of the QTc Interval and Cardiac Electrophysiology
In a thorough QT study, the mean increase in QTcF was 12.5 ms (90% two-sided upper confidence interval = 18.0 ms) after administration of a continuous dose of ONAPGO 6 mg/hr (maximum recommended infusion rate) in healthy subjects. A mean increase in QTcF of 14.6 ms (90% two-sided confidence interval = 20.1 ms) was observed at a dose and exposure similar to that expected with the maximum recommended total daily dosage of 98 mg. The maximum placebo-corrected increase in heart rate was 14.1 bpm (90% two-sided upper confidence interval = 17.4 bpm) at the dose and exposure similar to that expected with the maximum recommended total daily dose of 98 mg.
12.3 Pharmacokinetics
Absorption
After subcutaneous administration, apomorphine appears to have bioavailability equal to that of intravenous administration. Steady-state concentrations are reached in approximately two hours after initiation of a continuous dose. If an extra dose is administered at the initiation of the continuous dose [see Dosage and Administration (2.3)] , time to reach half (50%) of infusion steady-state concentrations can be shortened by 50-75%. If an extra dose is administered two hours or later following initiation of a continuous dose, the supplemental exposure from the extra dose reaches peak concentration in 20-40 minutes.
Distribution and Binding
The plasma-to-whole blood apomorphine concentration ratio is equal to one. Mean (range) apparent volume of distribution was 218 L (123 to 404 L). Protein binding in humans is 89% and concentration independent.
Elimination
The mean apparent clearance of apomorphine from plasma is 261 to 280 L/hr for ONAPGO with infusion rates ranging from 2 to 6 mg/hr. After administration of an extra dose, the mean elimination half-life is approximately 40 minutes.
Metabolism
Apomorphine metabolism is primarily via conjugation. Within 0.5 hours of administering a subcutaneous dose of 14C-apomorphine, only 8.3% of plasma radioactivity was apomorphine, while 83% was associated with the apomorphine sulfate, 3.5% with apomorphine glucuronide, and 1% with nor-apomorphine glucuronide.
Excretion
Eighty-six percent of the subcutaneously administered dose of 14C-apomorphine was recovered in the urine within 48 hours as apomorphine sulfate, apomorphine glucuronide and nor-apomorphine glucuronide. Another 4.6% of the administered dose was recovered in the feces over 144 hours as apomorphine sulfate, apomorphine glucuronide, and apomorphine.
Specific Populations
No clinically significant differences in the pharmacokinetics of apomorphine were observed based on age, gender, weight, duration of Parkinson's disease, levodopa dose, or duration of therapy.
Renal Impairment
In a study comparing patients with renal impairment (moderately impaired as determined by estimated creatinine clearance) to healthy matched volunteers, the AUC 0-infand C maxwere increased by approximately 16% and 50%, respectively, following a single subcutaneous administration of apomorphine into the abdominal wall. The mean time to peak concentrations and the mean terminal half-life of apomorphine were unaffected by the renal status of the individual. Studies in patients with severe renal impairment have not been conducted [see Dosage and Administration (2.5)and Use in Specific Populations (8.6)] .
Hepatic Impairment
In a study comparing patients with hepatic impairment (moderately impaired as determined by the Child-Pugh classification method) to healthy matched volunteers, the AUC 0-infand C maxvalues were increased by approximately 10% and 25%, respectively, following a single subcutaneous administration of apomorphine into the abdominal wall. Studies in patients with severe hepatic impairment have not been conducted [see Use in Specific Populations (8.7)] .
Drug Interaction Studies
Carbidopa/levodopa
Pharmacokinetics of levodopa were unchanged when subcutaneous apomorphine and levodopa were co-administered in patients. However, motor response differences were significant.
Ethanol and Nitroglycerin
Co-administration of low dose ethanol (0.3 g/kg), or nitroglycerin (0.4 mg) with an apomorphine injection dose of 6 mg in healthy individuals did not have a significant impact on the pharmacokinetics of apomorphine, but high dose ethanol (0.6 g/kg), equivalent to approximately 3 standardized alcohol- containing beverages, increased the C maxof apomorphine by about 63%. The hypotensive effect of apomorphine was increased by the concomitant use of alcohol or of sublingual nitroglycerin. When high-dose ethanol (0.6 g/kg) and subcutaneous apomorphine were concomitantly administered to healthy subjects, the mean largest decrease (the mean of each subject's largest drop in blood pressure measured within the 6-hour period following administration of subcutaneous apomorphine) for supine systolic and diastolic blood pressure was 9.1 mm Hg and 10.5 mm Hg, respectively. The mean largest standing systolic and diastolic blood pressure decrease was 11.3 mm Hg and 12.6 mm Hg, respectively. In some individuals, the decrease was as high as 61 mm Hg and 51 mm Hg, respectively, for standing systolic and diastolic blood pressure [see Warnings and Precautions (5.4), Drug Interactions (7.2, 7.3)].
Other Drugs Eliminated Via Hepatic Metabolism
Based upon an in vitrostudy, cytochrome P450 enzymes play a minor role in the metabolism of apomorphine. In vitrostudies have also demonstrated that drug interactions are unlikely due to apomorphine acting as a substrate, an inhibitor, or an inducer of cytochrome P450 enzymes.
COMT Interactions
A pharmacokinetic interaction of ONAPGO with catechol-O-methyl transferase (COMT) inhibitors or drugs metabolized by this route is unlikely because apomorphine appears not to be metabolized by COMT.
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Lifetime carcinogenicity studies of apomorphine were conducted in male (0.1, 0.3, or 0.8 mg/kg/day) and female (0.3, 0.8, or 2 mg/kg/day) rats. Apomorphine was administered by subcutaneous injection for 22 months or 23 months, respectively. In males, there was an increase in Leydig cell tumors at the highest dose tested. This finding is of questionable significance because the endocrine mechanisms believed to be involved in the production of Leydig cell tumors in rats are not relevant to humans. No drug-related tumors were observed in females. The highest doses tested in males and females are less than the maximum recommended human dose (MRHD) on a mg/m 2basis.
In a 26-week carcinogenicity study in p53-knockout transgenic mice, there was no evidence of carcinogenic potential when apomorphine was administered by subcutaneous injection at doses up to 20 mg/kg/day in males or 40 mg/kg/day in females.
Mutagenesis
Apomorphine was mutagenic in the in vitrobacterial reverse mutation (Ames) and the in vitromouse lymphoma tkassays. Apomorphine was clastogenic in the in vitrochromosomal aberration assay in human lymphocytes and in the in vitromouse lymphoma tkassay. Apomorphine was negative in the in vivomicronucleus assay in mice.
Impairment of Fertility
Apomorphine was administered subcutaneously at doses up to 3 mg/kg/day to male and female rats prior to and throughout the mating period and continuing in females through gestation day 6. There was no evidence of adverse effects on fertility or on early fetal viability. The highest dose tested is less than the MRHD on a mg/m 2basis. A significant decrease in testis weight was observed in a 39-week study in cynomolgus monkey at all subcutaneous doses tested (0.3, 1, or 1.5 mg/kg/day); the lowest dose tested is less than the MRHD on a mg/m 2basis.
In a published fertility study, apomorphine was administered to male rats at subcutaneous doses of 0.2, 0.8, or 2 mg/kg prior to and throughout the mating period. Fertility was reduced at the highest dose tested.
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
Study 1 (NCT02006121) was a multicenter, parallel-group, double-blind, randomized, placebo-controlled trial to evaluate the efficacy and safety of ONAPGO subcutaneous infusion in patients with Parkinson's disease who had motor fluctuations while receiving carbidopa/levodopa and other concomitant medications to treat PD. The study design included a double-blind, 12-week treatment period, inclusive of 1-4 weeks of dose titration and then continued treatment with study medication at an individualized, stable dosage. Patients then had the option to receive ONAPGO in a 52-week, open-label treatment period.
The modified intent-to-treat (mITT) population included 53 patients treated with ONAPGO and 51 patients who received placebo. At baseline, patients experienced OFF episodes averaging ≥3 hours per day. In the mITT population, the mean age was 63.4 years, 62% were male, and 100% were White. At baseline, all patients were taking at least one concomitant medication to treat PD (e.g., dopamine agonist 87%, COMT-inhibitor 58%, MAO-B inhibitor 40%, amantadine 27%) in addition to oral immediate or extended-release levodopa plus a dopa decarboxylase inhibitor. The mean duration of PD was 11.9 years in the ONAPGO-treated group and 10.8 years in the placebo-treated group.
During titration, adjustments in concomitant medications to treat PD were made when clinically indicated. All patients treated with ONAPGO in the double- blind study were maintained on levodopa.
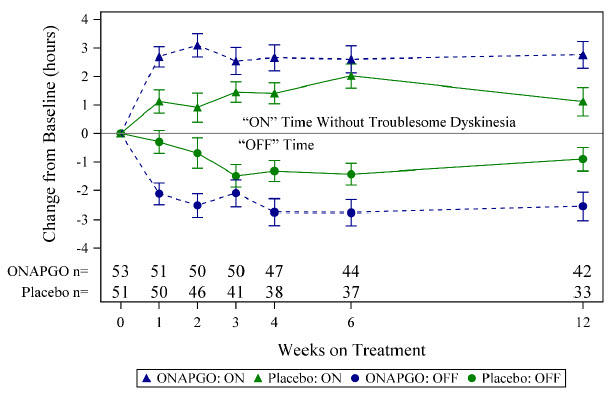
The primary efficacy endpoint for Study 1 was the change in total daily OFF time assessed from baseline to the end of the 12-week treatment period based on patient diaries. A key secondary endpoint was the change in daily ON time without troublesome dyskinesia from baseline to the end of the 12-week treatment period. There was a statistically significant reduction in the amount of daily OFF time in patients treated with ONAPGO compared to placebo (p=0.0114; see Table 2). There was also a statistically significant increase in daily ON time without troublesome dyskinesia in patients treated with ONAPGO compared to placebo (p=0.0188; see Table 3).
Table 2: Change From Baseline to Week 12 in Mean Total Daily OFF Time in Study 1 (mITT population)|
N |
Baseline (hours) |
LS Mean Change from Baseline at Week 12 |
LSD *vs Placebo | |
|---|---|---|---|---|
| ||||
|
Placebo |
51 |
6.72 ± 2.547 |
-0.90 ± 0.416 |
-- |
|
ONAPGO |
53 |
6.69 ± 2.224 |
-2.55 ± 0.487 |
-1.65 |
|
N |
Baseline (hours) |
LS Mean Change from Baseline at Week 12 |
LSD *vs Placebo | |
|---|---|---|---|---|
| ||||
|
Placebo |
51 |
8.64 ± 2.496 |
1.12 ± 0.500 |
-- |
|
ONAPGO |
53 |
8.56 ± 2.329 |
2.76 ± 0.471 |
1.64 |
In addition, the time course showed numerically greater improvement in daily OFF time and daily ON time without troublesome dyskinesia in patients treated with ONAPGO compared to placebo, at all post-baseline timepoints (Figure 2).
Figure 2: Mean Change from Baseline in Daily OFF Time and ON Time Without Troublesome Dyskinesia
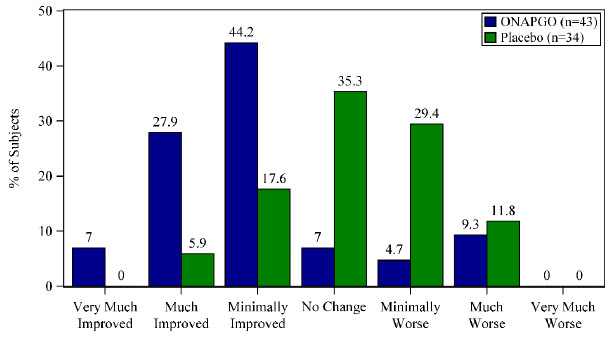
A patient reported outcome, the Patient Global Impression of Change (PGIC) was also assessed. The PGIC evaluates the change in Parkinson's disease symptoms as perceived by the patient in a seven-point single-item scale ranging from 'very much worse' to 'very much improved' (Figure 3).
Figure 3: Week 12 Patient Global Impression of Change
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
ONAPGO injection is supplied as one carton (NDC 27505-006-05) that contains five single-dose prefilled glass cartridges, each containing 98 mg/20 mL (4.9 mg/mL) apomorphine hydrochloride as a clear, almost colorless solution.
The ONAPGO Pump Kit, ONAPGO Cartridge Holders, and appropriate infusion sets are supplied separately.
16.2 Storage and Handling
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
INFORMATION FOR PATIENTS SECTION
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Administration Information
Refer patients to the Instructions for Use for complete administration instructions. Inform patients of aseptic technique and of subcutaneous administration site selection and rotation [see Dosage and Administration (2.4)].
Advise patients that a new single-dose cartridge and cartridge holder and a new infusion line should be used each day.
Advise patients that ONAPGO is intended only for subcutaneous use and must not be given intravenously because of the risk of serious complications, such as thrombus formation and pulmonary embolism due to crystallization [see Warnings and Precautions (5.1)] .
Hypersensitivity/Allergic Reactions
Advise patients that hypersensitivity/allergic reactions characterized by urticaria, rash, pruritus, and/or various manifestations of angioedema may occur because of ONAPGO or any of its excipients, including a sulfite (i.e., sodium metabisulfite). Inform patients with a sulfite sensitivity that they may experience various allergic-type reactions, including anaphylactic symptoms and life-threatening asthmatic attacks [see Warnings and Precautions (5.13)] . Advise patients who experience any hypersensitivity/allergic reaction to ONAPGO that they should not take ONAPGO again [see Contraindications (4)].
Nausea and Vomiting
Advise patients that they may experience nausea and vomiting, which may be severe. Advise patients that their ONAPGO dosage may be adjusted to start at 1mg/hr, and titration can be based upon effectiveness and tolerability. Treatment with an antiemetic that is a non-5HT3 antagonist may be used if needed. Oral trimethobenzamide 300 mg 3 times per day for 3 days prior to starting ONAPGO infusion has been used in clinical studies to help lessen these symptoms. Advise patients that ONAPGO taken with trimethobenzamide may increase the risk for somnolence, dizziness, and falls, and to consult their healthcare provider before discontinuing trimethobenzamide [see Warnings and Precautions (5.2)].
Falling Asleep Suddenly and Sedation/Sleepiness
Alert patients to the potential sedating effects of ONAPGO, including somnolence and falling asleep while engaged in activities of daily living. Instruct patients not to drive a car or engage in other potentially dangerous activities until they have gained sufficient experience with ONAPGO to gauge whether or not it affects their mental and/or motor performance adversely. Advise patients that if increased somnolence or episodes of falling asleep during activities of daily living (e.g., watching television, passenger in a car, etc.) occur, they should not drive or participate in potentially dangerous activities until they have contacted their physician [see Warnings and Precautions (5.3)].
Hypotension/Orthostatic Hypotension
Advise patients that they may develop postural (orthostatic) hypotension with or without symptoms such as dizziness, nausea, syncope, and sometimes sweating. Hypotension and/or orthostatic symptoms may occur more frequently during initial therapy or with an increase in dose at any time (cases have been seen after months of treatment). Instruct patients to rise slowly after sitting or lying down while using ONAPGO. Inform patients that alcohol and nitroglycerin (and possibly other vasodilators and antihypertensive medications) may worsen the potential effects of hypotension caused by ONAPGO [see Warnings and Precautions (5.4)]. Instruct patients ideally to lie down before taking sublingual nitroglycerin and to remain supine and avoid standing for at least 45 minutes after nitroglycerin. Instruct patients to avoid alcohol while using ONAPGO.
Falls
Alert patients that they may have increased risk for falling when using ONAPGO [see Warnings and Precautions (5.5)].
Infusion Site Reactions and Infections
Inform patients that infusion of ONAPGO may result in infusion site reactions, including, but not limited to nodules, erythema, bruising, and infection. Infusion site infections were reported in <5% of patients on ONAPGO in clinical trials [see Warnings and Precautions (5.6)and Adverse Reactions (6.1)] . Instruct patients to change the infusion site every day and to observe proper aseptic technique [see Dosage and Administration (2.4)and Instructions for Use] .
Hallucinations and/or Psychotic-Like Behavior
Inform patients that ONAPGO may cause hallucinations or other manifestations of psychotic-like behavior. Advise patients to inform their healthcare provider if they have a major psychotic disorder or are taking any treatments for psychosis. Patients with a major psychotic disorder should also be aware that many treatments for psychosis may decrease the effectiveness of ONAPGO [see Warnings and Precautions (5.7)] .
Dyskinesia
Inform patients that ONAPGO may cause and/or exacerbate pre-existing dyskinesia [see Warnings and Precautions (5.8)].
Hemolytic Anemia
Inform patients and caregivers that hemolytic anemia may occur and to contact their healthcare provider if they develop any signs or symptoms [see Warnings and Precautions (5.9)] .
Impulse Control / Compulsive Behaviors
Patients and their caregivers should be alerted to the possibility that they may experience intense urges to spend money uncontrollably, intense urges to gamble, increased sexual urges, binge eating and/or other intense urges and the inability to control these urges while using ONAPGO [see Warnings and Precautions (5.10)].
Cardiac Events
Inform patients that ONAPGO may cause cardiac (and cerebral) ischemia, and these outcomes could possibly be related to significant hypotension/orthostatic hypotension [see Warnings and Precautions (5.11)].
QTc Prolongation and Potential for Proarrhythmic Effects
Alert patients that ONAPGO may cause QTc prolongation and might produce proarrhythmic effects that could cause torsades de pointes and sudden death. Palpitations and syncope may signal the occurrence of an episode of torsades de pointes [see Warnings and Precautions (5.12)].
Priapism
Advise patients that ONAPGO may cause prolonged painful erections and that if this occurs, they should seek medical attention immediately [see Warnings and Precautions (5.15)]
SPL UNCLASSIFIED SECTION
ONAPGO Manufactured for: MDD US Operations, LLC, 9715 Key West Ave., Rockville, MD 20850.
MDD US Operations, LLC is a subsidiary of Supernus Pharmaceuticals, Inc.
ONAPGO is a trademark of BRITUSWIP LTD.
All trademarks are the property of their respective owners.
© 2025 MDD US Operations, LLC, a subsidiary of Supernus Pharmaceuticals Inc.
RA-ONG-V1
SPL PATIENT PACKAGE INSERT SECTION
|
This Patient Information has been approved by the U.S. Food and Drug Administration |
Issued: 2/2025 | |||
|
PATIENT INFORMATION | ||||
|
What is ONAPGO? | ||||
|
ONAPGO is a prescription medicine used to treat motor fluctuations (OFF episodes) in adults with advanced Parkinson's disease. | ||||
|
It is not known ifONAPGOis safe and effective in children. | ||||
|
Who should not use ONAPGO? | ||||
|
Do not use ONAPGO if you are: | ||||
| ||||
|
|
|
| |
|
What should I tell my healthcare provider before using ONAPGO? | ||||
|
Before you start usingONAPGO, tell your healthcare provider about all of your medical conditions, including if you: | ||||
| ||||
|
Tell your healthcare provider about all the medicines you take, including prescription and non-prescription (over-the-counter) medicines, vitamins, and herbal supplements. | ||||
|
ONAPGO and certain other medicines may affect each other and how they work. Using ONAPGO with other medicines can cause serious side effects. | ||||
| ||||
|
Know the medicines you take. Keep a list of them to show your healthcare provider or pharmacist when you get a new medicine. | ||||
|
How should I use ONAPGO? | ||||
| ||||
|
What should I avoid while using ONAPGO? | ||||
|
*Do notdrink alcohol while you are using ONAPGO. It can increase your chance of developing serious side effects. *Do nottake medicines that make you sleepy while you are using ONAPGO. *Do notdrive, operate machinery, or do other dangerous activities until you know how ONAPGO affects you. *Do notchange your body position too fast. Get up slowly from sitting or lying. ONAPGO can lower your blood pressure and cause dizziness or fainting. | ||||
|
What are the possible side effects of ONAPGO? | ||||
|
ONAPGO may cause serious side effects, including: | ||||
|
***blood clots.**Infusing ONAPGO into a vein (intravenous) can cause blood clots.Do notinfuse ONAPGO in your vein. ***nausea and vomiting are common side effects.**Nausea and vomiting, which may be serious or severe, can happen with ONAPGO. Your healthcare provider may prescribe medicine (trimethobenzamide) to help decrease nausea and vomiting. Follow your healthcare providers instructions on how to take and when to stop this medicine. ***sleepiness or falling asleep during the day is a common side effect and may be serious.**Some people treated with ONAPGO may get sleepy during the day or fall asleep without warning while doing everyday activities such as talking, eating, or driving a car. ***dizziness is a common side effect and may be serious.**ONAPGO can lower your blood pressure and cause dizziness. Dizziness can happen when ONAPGO treatment is started or when the ONAPGO dose is increased.Do notget up too fast from sitting or after lying down, especially if you have been sitting or lying down for a long period of time. ***falls.**The changes that can happen with PD, and the effects of some PD medicines as well as the effects of trimethobenzamide, can increase the risk of falling. ONAPGO may also increase your risk of falling. ***infusion site reaction is a common side effect that may be serious.**Infusion site reactions and infections including infusion site nodules, redness, bruising, swelling, rash, and itching may happen during treatment with ONAPGO. ***hallucinations or psychotic-like behavior.**ONAPGO can cause or worsen psychotic-like behavior including hallucinations (seeing or hearing things that are not real), confusion, excessive suspicion, aggressive behavior, agitation, delusional beliefs (believing things that are not real), and disorganized thinking. ***sudden uncontrolled movements (dyskinesia) are a common side effect and may be serious.**Some people with PD may get sudden, uncontrolled movements after treatment with some PD medicines. ONAPGO can cause or make dyskinesia worse. ***low red blood cells (hemolytic anemia).**Tell your healthcare provider if you have any of the following signs or symptoms: you become pale, fast heartbeat, feel more tired or weaker than usual, skin or eyes look yellow, chest pain, shortness of breath or trouble breathing, dark-colored urine, fever, dizziness, or confusion. ***strong (intense) urges.**Some people with PD have reported new or increased gambling urges, increased sexual urges, and other intense urges, while taking PD medicines, including ONAPGO. ***heart problems.**If you have shortness of breath, fast heartbeat, or chest pain while taking ONAPGO, call your healthcare provider or get emergency help right away. ***serious heart rhythm changes (QT prolongation).**Tell your healthcare provider right away if you have a change in your heartbeat (a fast or irregular heartbeat), or if you faint. ***allergic reaction.**An allergic reaction can happen when using ONAPGO. Tell your healthcare provider or get medical help right away if you get any of these symptoms: hives, itching, rash, swelling of the eyes and tongue, or trouble breathing. ***tissue changes (fibrotic complications).**Some people have had changes in the tissues of their pelvis, lungs, and heart valves when taking medicines called non-ergot derived dopamine agonists like ONAPGO. *prolonged painful erections (priapism). ONAPGO may cause prolonged, painful erections in some people. If you have an erection that lasts more than 4 hours you should call your healthcare provider or go to the nearest hospital emergency room right away. | ||||
|
Other common side effects of ONAPGO include: | ||||
| ||||
|
Tell your healthcare provider if you have any side effect that bothers you or that does not go away. | ||||
|
These are not all the possible side effects of ONAPGO. For more information, ask your healthcare provider or pharmacist. | ||||
|
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. | ||||
|
How should I store ONAPGO? | ||||
| ||||
|
Keep ONAPGO and all medicines out of the reach of children. | ||||
|
General information about the safe and effective use of ONAPGO. | ||||
|
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use ONAPGO for a condition for which it was not prescribed. Do not give ONAPGO to other people, even if they have the same symptoms that you have. It may harm them. | ||||
|
You can ask your healthcare provider or pharmacist for information about ONAPGO that is written for health professionals. | ||||
|
What are the ingredients in ONAPGO? | ||||
|
**Active ingredient:**apomorphine hydrochloride | ||||
|
**Inactive ingredients:**hydrochloric acid, sodium metabisulfite in water for injection. | ||||
|
Manufactured for: MDD US Operations, LLC, 9715 Key West Ave., Rockville, MD 20850. | ||||
|
MDD US Operations, LLC is a subsidiary of Supernus Pharmaceuticals, Inc. | ||||
|
MDD US Operations, LLC is the exclusive licensee and distributor of ONAPGO in the United States and Its territories. | ||||
|
ONAPGO is a trademark of BRITUSWIP LTD. | ||||
|
©2025MDD US Operations, LLC, a subsidiary of Supernus Pharmaceuticals, Inc. | ||||
|
For more information, go toONAPGO.comor call1-833-366-2746 |
RA-ONG-PPI-V1
INSTRUCTIONS FOR USE SECTION
Healthcare Provider
INSTRUCTIONS FOR USE
ONAPGO™ (on-AP-goh)

This Instructions for Use contains information for healthcare providers on how to program the infusion pump to administer ONAPGO (apomorphine hydrochloride).
Please see the Important Safety Information, full Prescribing Information, and Patient Informationfor ONAPGO.
MDD US Operations, LLC
ONAPGO Infusion System
|
Indication for Use |
The ONAPGO Infusion Pump is for the subcutaneous infusion of ONAPGO (apomorphine hydrochloride). ONAPGO is indicated for the treatment of motor fluctuations in adults with advanced Parkinson's disease (PD).
It must be used only by individuals who have received instruction and training on its operations and on the correct, safe procedures. If patients are unable to give treatment independently, they must be given assistance and supervision.
Only the accessories supplied by Cane' S.p.A. (plastic cartridge holder and supplies provided in the infusion pump kit) may be used in conjunction with this pump. The pump must be programmed by an adequately trained healthcare provider and/or a Supernus Pharmaceuticals/MDD US Operations Clinical Nurse Navigator (clinical nurse navigator ).
|
Introduction to the Infusion System |
Below are the common terms used throughout this Instructions for Use.
***Pump:**controls the rate and amount of ONAPGO delivered to the body. It is programmed with the patient's prescription and displays the status of medicine delivery. ***Priming:**refers to the task of removing all air from the Infusion Line (fluid pathway) before the infusion line is connected to the body. ***Flow Rate:**the constant flow of ONAPGO given to the body over an extended period of time. The flow rate is expressed as milligrams per hour (mg/hr). ***Infusion Time:**the total time that ONAPGO is infused per day. ***Extra Dose (+ Dose):**a boost of ONAPGO (bolus dose) given over a short period of time in addition to the prescribed flow rate. ***Extra Dose (+ Dose) Lock:**the amount of time before another extra dose can be given. ***Pump Settings:the patient's prescribed Flow Rate, Maximum Infusing Time Per Day,+Dose Quantity,+Dose Volume, and+**Dose Lock. These settings can only be changed by a Healthcare Provider and/or Supernus Clinical Nurse Navigator.
|
Pump Warnings and Precautions |
 WARNINGS:
WARNINGS:
*Do notgive a patient a pump without checking the prescription. Always check that the pump Settings match the patient's prescription before giving the pump to a patient. *Do notstart an infusion without confirming the patient's prescription. If the pump settings do not match the prescription, do not allow the patient to use the pump. Reprogram the pump to match the prescription. *Do notgive a patient more than 98 mg of ONAPGO over a 24-hour period. *Do notdisclose the pump's security codes or other information to the patient. It would allow them access to the programming functions.
- Use ONAPGO drug cartridges with the ONAPGO pump only.
 PRECAUTIONS:
PRECAUTIONS:
*Do notuse sharp objects to press the pump buttons. Only use your fingertips. *Do notuse a damaged pump. If you have any concerns about the correct functioning of the pump, and/or how to respond to an error contact your customer support representative.
|
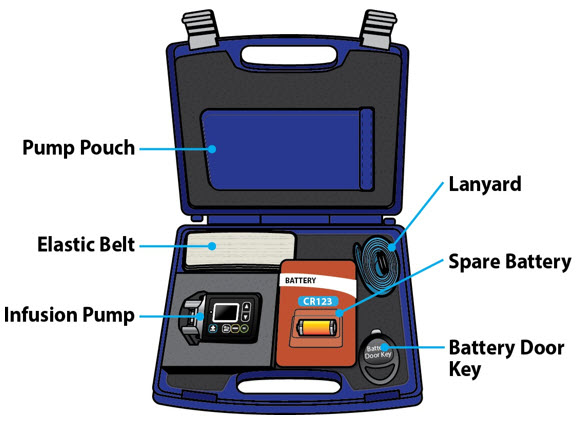
Pump Kit (Figure A) |
|
Pump Diagram (Figures B, C, and D) |
|
|
| |
|
|
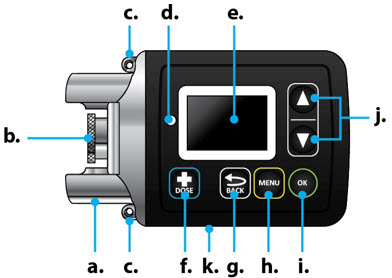 Figure B
Figure B
 Figure C
Figure CAll buttons will respond with a single press. If the screen is dark, press the
UP ARROW (  ) to
wake up the screen.
) to
wake up the screen.
|
Item |
Pump Feature |
Description |
|---|---|---|
|
a |
Cartridge Connection |
Area where assembled glass drug cartridge and plastic cartridge holder is attached to the pump. |
|
b |
Pump Pusher |
Pushes ONAPGO from the glass drug cartridge into the Infusion Line. |
|
c |
Neck Lanyard Clips |
Slots to clip on the lanyard. |
|
d |
LED |
Lights up when an error cannot be displayed on the screen. |
|
e |
Screen |
Where messages and menus appear. |
|
f |
|
**+**DOSE button gives an extra dose (if prescribed). |
|
g |
|
BACK button allows you to return to a previous screen, menu, or cancel an action. |
|
h |
|
MENU button allows you to access the menus. |
|
i |
|
OK button allows you to confirm menu selections or go on to the next value. |
|
j |
|
UP and DOWN ARROW buttons allow you to scroll through menus. |
|
k |
Battery Door |
Door to access the battery. |





|
Pump Screen Icons |
The following table shows Icons that appear on the Pump screen.
|
Icon |
Name |
Description | |
|---|---|---|---|
|
|
Back Arrow |
The back arrow is shown when checking the pump settings. This icon is used to show that pressing the BACK button will return to a previous screen (Item 'g' in Figure B). | |
|
|
Caution |
Caution is shown when an error or alarm is occurring. | |
|
|
Check Mark |
A check mark is shown when the Pump successfully completes a task. | |
|
|
Droplet |
A blinking droplet is shown on the Infusing Screen when an infusion is on. | |
|
|
Dead Battery |
The dead battery is shown when the Pump battery is dead and must be replaced. | |
|
|
Low Battery |
The low battery is shown when the pump battery is low and should be replaced before the next infusion. | |
|
|
OK Arrow |
The OK arow is shown when checking the pump settings. This icon is used to show that pressing the OK button will confirm a selection or go on to the next value (Item 'i' in Figure B). | |
|
|
Padlock |
Padlock is shown when the**+**Dose (extra dose) is not available. |
|
|
|
Pause |
Pause is shown when the infusion is paused. | |
|
|
**+**Dose |
A**+symbol refers to the extra dose (+**Dose) function. |











Programming the ONAPGO Pump
The pump cannot be programmed while infusing.
The pump settings should be programmed according to the patient's prescription before they receive the pump.
|
Settings Overview |
When programming the pump, a flashing value is one that you may edit. The table below describes the default pump settings and range of values to which the pump can be programmed. See the Prescribing Information for the recommended dosage regimen, including the recommended flow rate (i.e., 1 mg/hr to 6 mg/hr), infusion time (i.e., generally over 16 waking hours), and extra doses (i.e., no more than 3 per day).
|
Icon |
Default Pump Setting |
Range of Values |
Increments |
Refer To |
|---|---|---|---|---|
|
Time |
Factory setting |
12:00 AM - 11:59 PM |
N/A |
Step 3.1 |
|
Date |
Factory setting |
mm/dd/yy |
N/A |
Step 3.2 |
|
Flow Rate |
1 mg/hr |
1 - 8 mg/hr |
0.5 mg/hr |
Step 3.3 |
|
Infusion Time |
1 hr |
1 - 24 hr |
1 hr |
Step 3.4 |
|
**+**Doses/Day |
0 |
0 - 5 |
1 |
Step 3.5 |
|
**+**Dose |
0 mg |
0.5 - 4 mg |
0.5 mg |
Step 3.6 |
|
**+**Dose Lock |
3 hr |
0 - 24 hr |
30 min |
Step 3.7 |
|
Step 1: Access Pump Settings |
|
Step 1.1 |
|
|
When the pump wakes up, the screen will say Infusion Off (Figure F). |
|
|
Step 1.2 |
|
|
Keep holding both buttons until the password screen appears. |
|
 ) to wake it up
(Figure E).
) to wake it up
(Figure E). Figure E
Figure E
 ). While continuing
to hold, press and hold the UP ARROW at the same time (Figure G), until a
password input screen appears (Figure H).
). While continuing
to hold, press and hold the UP ARROW at the same time (Figure G), until a
password input screen appears (Figure H). ) and OK button (
) and OK button (
 ).
).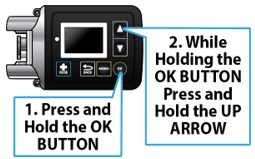
 Figure H
Figure H|
Step 2: Enter Password |
Important Information:
**** Do
notdisclose the pump's security codes or other information to the patient.
It would allow them access to the programming functions.
Do
notdisclose the pump's security codes or other information to the patient.
It would allow them access to the programming functions.
|
Step 2.1 |
|
|
Step 2.2 |
|
|
When the correct password has been entered, press the OK button ( |
|

 ) to change the
values on the Password screen (Figure J). Flashing values indicate that they
are currently being edited. When the selected number matches the pump
password, press the OK button
) to change the
values on the Password screen (Figure J). Flashing values indicate that they
are currently being edited. When the selected number matches the pump
password, press the OK button ) to proceed to
the next number. Repeat this process for all 4 numbers.
) to proceed to
the next number. Repeat this process for all 4 numbers. Figure J
Figure J ) to proceed to the Time
screen (Figure K).
) to proceed to the Time
screen (Figure K).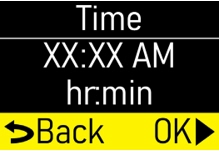 Figure K
Figure K|
Step 3: Program Pump Settings |
If this is the first time the pump will be programmed, the existing values will reflect the default factory settings (Page 8).
For any subsequent programming, the values will reflect the previously programmed patient prescription.
The settings will need to be changed to match the time, date, and patient's prescription.
|
Step 3.1 |
|
|
When the Time is correct, press the OK button (
|
|
|
Step 3.2 |
|
|
When the date is correct, press the OK button (
|
|
|
Step 3.3 |
|
|
When the flow rate is correct, press the OK button (
|
|
|
**Note:**If you are prescribing above the recommended flow rate, a Verify
screen will appear (Figure R). |
|
|
Step 3.4 |
|
|
When the infusion time is correct, press the OK button (
|
|
|
**Note:**If you are prescribing above the recommended infusion time, a Verify
screen will appear (Figure U). |
|
|
Step 3.5 |
|
|
When the**+Doses/Day (extra doses/ day) number is correct, press the OK
button ( |
|
|
**Note:If you are prescribing above the recommended+**Doses/Day, a Verify
screen will appear (Figure X). |
|
|
Step 3.6 |
|
|
When the**+**Dose (extra dose) value is correct, press the OK button (
|
|
|
**Note:**If you are prescribing above the recommended extra doses, a Verify
screen will appear (Figure AA). Press the OK button (
|
|
|
Step 3.7 |
|
|
When the + Dose (extra dose) lock time is correct, press the OK button (
|
|
|
Step 3.8 |
|
|
Continue pressing the DOWN ARROW (
|
|
|
Step 3.9 |
|
|
When the pump is done saving, the Infusion Off screen will appear (Figure AG). |
|
 ) to change the
hour. As the hour is adjusted, the AM and PM will also change. When the hour
and AM/PM are correct, press the OK button (
) to change the
hour. As the hour is adjusted, the AM and PM will also change. When the hour
and AM/PM are correct, press the OK button (
 ) to change the
minutes (Figure L). Use the UP and DOWN ARROWS (
) to change the
minutes (Figure L). Use the UP and DOWN ARROWS (
 ) to change the
minutes.
) to change the
minutes.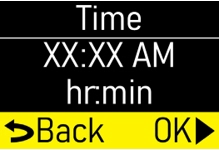 Figure L
Figure L ) to proceed to the
Date screen (Figure M) Step 3.2.
) to proceed to the
Date screen (Figure M) Step 3.2. Figure M
Figure M ) to change the
month and press the OK button (
) to change the
month and press the OK button (
 ) to continue to
change the day and year (Figure N).
) to continue to
change the day and year (Figure N). Figure N
Figure N ) to proceed to the
Flow Rate screen (Figure O) Step 3.3.
) to proceed to the
Flow Rate screen (Figure O) Step 3.3. Figure O
Figure O ) to change the
flow rate (Figure P).
) to change the
flow rate (Figure P). Figure P
Figure P ) to proceed to the
Infusion Time screen (Figure Q) Step 3.4.
) to proceed to the
Infusion Time screen (Figure Q) Step 3.4. Figure Q
Figure Q ) to proceed or
press the BACK button (
) to proceed or
press the BACK button (
 ) to edit the flow
rate.
) to edit the flow
rate. Figure R
Figure R ) to change the
Infusion Time (length of time that infusion will run) (Figure S).
) to change the
Infusion Time (length of time that infusion will run) (Figure S). Figure S
Figure S ) to proceed to the
) to proceed to the Figure T
Figure T ) to proceed or
press the BACK button (
) to proceed or
press the BACK button (
 ) to edit the
infusion time.
) to edit the
infusion time. Figure U
Figure U ) to change the
number of allowable**+**Doses (extra doses) that can be delivered per Day
(Figure V).
) to change the
number of allowable**+**Doses (extra doses) that can be delivered per Day
(Figure V). ) to proceed to the
**+Dose screen (Figure W) Step 3.6. If no+Doses/Day (extra doses/day)
are prescribed, the subsequent+Dose and+**Dose Lock screen values
cannot be changed.
) to proceed to the
**+Dose screen (Figure W) Step 3.6. If no+Doses/Day (extra doses/day)
are prescribed, the subsequent+Dose and+**Dose Lock screen values
cannot be changed. Figure V
Figure V ) to
proceed to the+**Dose screen (Figure W) Step 3.6.
) to
proceed to the+**Dose screen (Figure W) Step 3.6.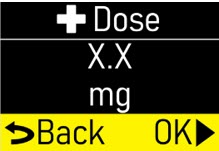 Figure W
Figure W ) to proceed or
press the BACK button (
) to proceed or
press the BACK button (
 ) to edit the
**+**Doses/Day (extra doses/day).
) to edit the
**+**Doses/Day (extra doses/day).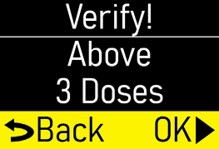 Figure X
Figure X ) to change the
**+**Dose (Extra Dose) value (mg) (Figure Y).
) to change the
**+**Dose (Extra Dose) value (mg) (Figure Y). ) to proceed to the
**+**Dose Lock screen (Figure Z) Step 3.7.
) to proceed to the
**+**Dose Lock screen (Figure Z) Step 3.7.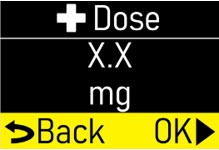 Figure Y
Figure Y ) to proceed to the
**+**Dose Lock screen (Figure Z) Step 3.7.
) to proceed to the
**+**Dose Lock screen (Figure Z) Step 3.7.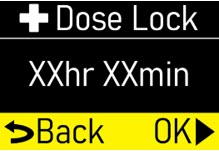 Figure Z
Figure Z ) to proceed or
press the BACK button (
) to proceed or
press the BACK button (
 ) to edit the
**+**Dose (extra dose).
) to edit the
**+**Dose (extra dose).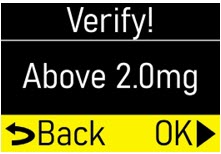 Figure AA
Figure AA ) to change the +
Dose Lock (extra dose lock) time (time patient must wait before another extra
dose) (Figure AB).
) to change the +
Dose Lock (extra dose lock) time (time patient must wait before another extra
dose) (Figure AB). ) to proceed to the
Verify Rx screen (Figure AC) Step 3.8.
) to proceed to the
Verify Rx screen (Figure AC) Step 3.8.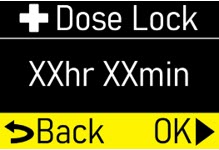 Figure AB
Figure AB ) to proceed to the
Verify Rx screen (Figure AC) Step 3.8.
) to proceed to the
Verify Rx screen (Figure AC) Step 3.8.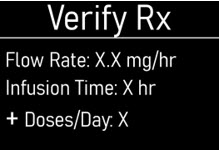 Figure AC
Figure AC ) to confirm that
each pump setting programmed matches the patient's prescription.
) to confirm that
each pump setting programmed matches the patient's prescription.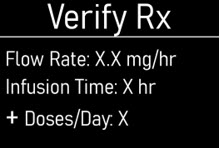 Figure AD
Figure AD ) until the Back/OK
row is highlighted (Figure AE).
) until the Back/OK
row is highlighted (Figure AE). Figure AE
Figure AE ) to save
the pump settings (Figure AF).
) to save
the pump settings (Figure AF). ) to go back to the
setting and adjust accordingly.
) to go back to the
setting and adjust accordingly. Figure AF
Figure AF Figure AG
Figure AGSymbols Used on the ONAPGO Pump
|
|
**Caution:**Consult accompanying documents for important safety-related information. |
|
|
CF Applied Part, refer to Technical Manual for more information. |
|
|
**Caution:**Consult Instructions for Use. |
|
|
Do not use in or next to a Magnetic Resonance Imaging (MRI) medical device. |
|
|
Ingress Protection (IP) rating. |
|
|
Prescription device. |
|
|
The pump is to only be used with a CR123A battery. |







**Note:**The symbols displayed on the product label is reduced and simplified compared to the specifications in the reference standard CENELEC EN50419.
Limited Warranty
The pump is covered by a manufacturer's warranty for three (3) years. After this period, the manufacturer shall not be responsible for any repairs.
The manufacturer shall not be liable for damage to persons or property after a pump lifetime of three (3) years.
Contact & Support
For help and additional information on the pump or system, contactCustomer Support at 1-833-3ONAPGO (1-833-366-2746).
Manufactured for:
MDD US Operations, LLC, a
subsidiary of Supernus Pharmaceuticals, Inc.
Rockville, MD 20850
MDD US Operations, LLC is the exclusive licensee and distributor of ONAPGO in the United States and Its territories.
©2025. ONAPGO is a registered trademark of BRITUSWIP LTD.
Version 8
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: 06/2025