
Erythromycin Ethylsuccinate
To reduce the development of drug-resistant bacteria and maintain the effectiveness of erythromycin ethylsuccinate and other antibacterial drugs, erythromycin ethylsuccinate should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.
3d80f96e-3bbe-4fa5-89a8-694c61dd5e8f
HUMAN PRESCRIPTION DRUG LABEL
Jun 20, 2025
ANI Pharmaceuticals, Inc.
DUNS: 145588013
Products 2
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Erythromycin Ethylsuccinate
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (9)
Erythromycin Ethylsuccinate
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (9)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
Erythromycin Ethylsuccinate for Oral Suspension USP, Erythromycin activity
400 mg per 5 mL when reconstituted
NDC 62559-631-01
Rx only
100 mL (when mixed)
**
 **
**
PRECAUTIONS SECTION
PRECAUTIONS
General
Prescribing erythromycin ethylsuccinate in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Since erythromycin is principally excreted by the liver, caution should be exercised when erythromycin is administered to patients with impaired hepatic function. (SeeCLINICAL PHARMACOLOGY andWARNINGS sections.)
Exacerbation of symptoms of myasthenia gravis and new onset of symptoms of myasthenic syndrome have been reported in patients receiving erythromycin therapy.
There have been reports of infantile hypertrophic pyloric stenosis (IHPS) occurring in infants following erythromycin therapy. In one cohort of 157 newborns who were given erythromycin for pertussis prophylaxis, seven neonates (5%) developed symptoms of non-bilious vomiting or irritability with feeding and were subsequently diagnosed as having IHPS requiring surgical pyloromyotomy. A possible dose-response effect was described with an absolute risk of IHPS of 5.1% for infants who took erythromycin for 8-14 days and 10% for infants who took erythromycin for 15-21 days.2 Since erythromycin may be used in the treatment of conditions in infants which are associated with significant mortality or morbidity (such as pertussis or neonatal Chlamydia trachomatis infections), the benefit of erythromycin therapy needs to be weighed against the potential risk of developing IHPS. Parents should be informed to contact their physician if vomiting or irritability with feeding occurs.
Prolonged or repeated use of erythromycin may result in an overgrowth of nonsusceptible bacteria or fungi. If superinfection occurs, erythromycin should be discontinued and appropriate therapy instituted.
When indicated, incision and drainage or other surgical procedures should be performed in conjunction with antibiotic therapy. Observational studies in humans have reported cardiovascular malformations after exposure to drug products containing erythromycin during early pregnancy.
Information for Patients
Patients should be counseled that antibacterial drugs including erythromycin ethylsuccinate should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When erythromycin ethylsuccinate is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by erythromycin ethylsuccinate or other antibacterial drugs in the future.
Diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Drug Interactions
Theophylline: Erythromycin use in patients who are receiving high doses of theophylline may be associated with an increase in serum theophylline levels and potential theophylline toxicity. In case of theophylline toxicity and/or elevated serum theophylline levels, the dose of theophylline should be reduced while the patient is receiving concomitant erythromycin therapy.
There have been published reports suggesting that when oral erythromycin is given concurrently with theophylline there is a decrease in erythromycin serum concentrations of approximately 35%. The mechanism by which this interaction occurs is unknown. The decrease in erythromycin concentrations due to co- administration of theophylline could result in subtherapeutic concentrations of erythromycin.
Hypotension, bradyarrhythmias, and lactic acidosis have been observed in patients receiving concurrent verapamil, belonging to the calcium channel blockers drug class.
Concomitant administration of erythromycin and digoxin has been reported to result in elevated digoxin serum levels.
There have been reports of increased anticoagulant effects when erythromycin and oral anticoagulants were used concomitantly. Increased anticoagulation effects due to interactions of erythromycin with various oral anticoagulants may be more pronounced in the elderly.
Erythromycin is a substrate and inhibitor of the 3A isoform subfamily of the cytochrome p450 enzyme system (CYP3A). Coadministration of erythromycin and a drug primarily metabolized by CYP3A may be associated with elevations in drug concentrations that could increase or prolong both the therapeutic and adverse effects of the concomitant drug. Dosage adjustments may be considered, and when possible, serum concentrations of drugs primarily metabolized by CYP3A should be monitored closely in patients concurrently receiving erythromycin.
The following are examples of some clinically significant CYP3A based drug interactions. Interactions with other drugs metabolized by the CYP3A isoform are also possible. The following CYP3A based drug interactions have been observed with erythromycin products in post-marketing experience:
Ergotamine/dihydroergotamine: Post-marketing reports indicate that co- administration of erythromycin with ergotamine or dihydroergotamine has been associated with acute ergot toxicity characterized by vasospasm and ischemia of the extremities and other tissues including the central nervous system. Concomitant administration of erythromycin with ergotamine or dihydroergotamine is contraindicated (seeCONTRAINDICATIONS).
Triazolobenzodiazepines: (such as triazolam and alprazolam) and Related Benzodiazepines: Erythromycin has been reported to decrease the clearance of triazolam and midazolam, and thus, may increase the pharmacologic effect of these benzodiazepines.
HMG-CoA Reductase Inhibitors: Erythromycin has been reported to increase concentrations of HMG-CoA reductase inhibitors (e.g., lovastatin and simvastatin). Rare reports of rhabdomyolysis have been reported in patients taking these drugs concomitantly.
Sildenafil (Viagra): Erythromycin has been reported to increase the systemic exposure (AUC) of sildenafil. Reduction of sildenafil dosage should be considered. (See Viagra package insert.)
There have been spontaneous or published reports of CYP3A based interactions of erythromycin with cyclosporine, carbamazepine, tacrolimus, alfentanil, disopyramide, rifabutin, quinidine, methylprednisolone, cilostazol, vinblastine, and bromocriptine.
Concomitant administration of erythromycin with cisapride, pimozide, astemizole, or terfenadine is contraindicated. (SeeCONTRAINDICATIONS.)
In addition, there have been reports of interactions of erythromycin with drugs not thought to be metabolized by CYP3A, including hexobarbital, phenytoin, and valproate.
Erythromycin has been reported to significantly alter the metabolism of the nonsedating antihistamines terfenadine and astemizole when taken concomitantly. Rare cases of serious cardiovascular adverse events, including electrocardiographic QT/QTc interval prolongation, cardiac arrest, torsades de pointes, and other ventricular arrhythmias have been observed. (See CONTRAINDICATIONS.) In addition, deaths have been reported rarely with concomitant administration of terfenadine and erythromycin.
There have been post-marketing reports of drug interactions when erythromycin was co-administered with cisapride, resulting in QT prolongation, cardiac arrhythmias, ventricular tachycardia, ventricular fibrillation, and torsades de pointes most likely due to inhibition of hepatic metabolism of cisapride by erythromycin. Fatalities have been reported. (SeeCONTRAINDICATIONS.)
Colchicine: Colchicine is a substrate for both CYP3A4 and the efflux transporter P-glycoprotein (P-gp). Erythromycin is considered a moderate inhibitor of CYP3A4. A significant increase in colchicine plasma concentration is anticipated when co-administered with moderate CYP3A4 inhibitors such as erythromycin. If co-administration of colchicine and erythromycin is necessary, the starting dose of colchicine may need to be reduced, and the maximum colchicine dose should be lowered. Patients should be monitored for clinical symptoms of colchicine toxicity (seeWARNINGS).
Drug/Laboratory Test Interactions
Erythromycin interferes with the fluorometric determination of urinary catecholamines.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term oral dietary studies conducted with erythromycin stearate in rats up to 400 mg/kg/day and in mice up to 500 mg/kg/day (approximately 1-2 fold of the maximum human dose on a body surface area basis) did not provide evidence of tumorigenicity. Erythromycin stearate did not show genotoxic potential in the Ames, and mouse lymphoma assays or induce chromosomal aberrations in CHO cells. There was no apparent effect on male or female fertility in rats treated with erythromycin base by oral gavage at 700 mg/kg/day (approximately 3 times the maximum human dose on a body surface area basis).
Pregnancy
Teratogenic Effects.
There is no evidence of teratogenicity or any other adverse effect on reproduction in female rats fed erythromycin base by oral gavage at 350 mg/kg/day (approximately twice the maximum recommended human dose on a body surface area) prior to and during mating, during gestation, and through weaning. No evidence of teratogenicity or embryotoxicity was observed when erythromycin base was given by oral gavage to pregnant rats and mice at 700 mg/kg/day and to pregnant rabbits at 125 mg/kg/day (approximately 1-3 times the maximum recommended human dose).
Labor and Delivery
The effect of erythromycin on labor and delivery is unknown.
Nursing Mothers
Erythromycin is excreted in human milk. Caution should be exercised when erythromycin is administered to a nursing woman.
Pediatric Use
SeeINDICATIONS AND USAGE andDOSAGE AND ADMINISTRATION sections.
Geriatric Use
Elderly patients, particularly those with reduced renal or hepatic function, may be at increased risk for developing erythromycin-induced hearing loss. (SeeADVERSE REACTIONS andDOSAGE AND ADMINISTRATION).
Elderly patients may be more susceptible to the development of torsades de pointes arrhythmias than younger patients. (SeeWARNINGS).
Elderly patients may experience increased effects of oral anticoagulant therapy while undergoing treatment with erythromycin. (SeePRECAUTIONS - Drug Interactions).
Erythromycin ethylsuccinate for oral suspension 200 mg/5 mL contains 106.9 mg (4.6 mEq) of sodium per individual dose.
Erythromycin ethylsuccinate for oral suspension 400 mg/5 mL contains 106.9 mg (4.6 mEq) of sodium per individual dose.
Based on the 200 mg/5 mL strength, at the usual recommended doses, adult patients would receive a total of 855.2 mg/day (37.2 mEq) of sodium. Based on the 400 mg/5 mL strength, at the usual recommended doses, adult patients would receive a total of 427.6 mg/day (18.6 mEq) of sodium. The geriatric population may respond with a blunted natriuresis to salt loading. This may be clinically important with regard to such diseases as congestive heart failure.
OVERDOSAGE SECTION
OVERDOSAGE
In case of overdosage, erythromycin should be discontinued. Overdosage should be handled with the prompt elimination of unabsorbed drug and all other appropriate measures should be instituted.
Erythromycin is not removed by peritoneal dialysis or hemodialysis.
To report SUSPECTED ADVERSE REACTIONS, contact ANI Pharmaceuticals, Inc. at 1-855-204-1431 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
HOW SUPPLIED SECTION
HOW SUPPLIED
Erythromycin Ethylsuccinate for Oral Suspension USP, 200 mg/5 mL is supplied in bottles of 100 mL (NDC 62559-630-01).
Erythromycin Ethylsuccinate for Oral Suspension USP, 400 mg/5 mL is supplied in bottles of 100 mL (NDC 62559-631-01).
Recommended Storage:
Store Erythromycin Ethylsuccinate for Oral Suspension USP, 200 mg/5 mL and 400 mg/5 mL, prior to mixing, below 86°F (30°C). After reconstitution, Erythromycin Ethylsuccinate for Oral Suspension USP, 200 mg/5 mL and 400 mg/5 mL must be stored at or below 77°F (25°C) and used within 35 days; refrigeration is not required.
REFERENCES
Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association: Prevention of Rheumatic Fever. Circulation. 78(4):1082-1086, October 1988.
Honein, M.A., et. al.: Infantile hypertrophic pyloric stenosis after pertussis prophylaxis with erythromycin: a case review and cohort study. The Lancet 1999;354 (9196): 2101-5.
Manufactured by:
ANI Pharmaceuticals, Inc.
Baudette, MN 56623
![]()
10147 Rev 06/25
DESCRIPTION SECTION
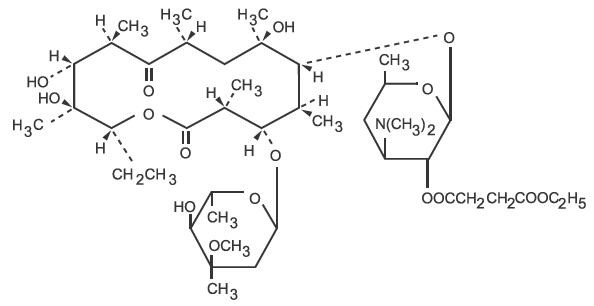
DESCRIPTION
Erythromycin is produced by a strain of Saccharopolyspora erythraea (formerly Streptomyces erythraeus) and belongs to the macrolide group of antibiotics. It is basic and readily forms salts with acids. The base, the stearate salt, and the esters are poorly soluble in water. Erythromycin ethylsuccinate is an ester of erythromycin suitable for oral administration. Erythromycin ethylsuccinate is known chemically as erythromycin 2'-(ethylsuccinate). The molecular formula is C43H75NO16 and the molecular weight is 862.06. The structural formula is:
Erythromycin Ethylsuccinate for Oral Suspension USP, 200 mg/5 mL when reconstituted with water, forms a suspension containing erythromycin ethylsuccinate equivalent to 200 mg erythromycin per 5 mL (teaspoonful) or 100 mg per 2.5 mL (dropperful) with an appealing cherry flavor. Erythromycin Ethylsuccinate for Oral Suspension USP, 400 mg/5 mL when reconstituted with water, forms a suspension containing erythromycin ethylsuccinate equivalent to 400 mg of erythromycin per 5 mL (teaspoonful) with an appealing cherry flavor.
These products are intended primarily for pediatric use but can also be used in adults.
Inactive Ingredients
Erythromycin Ethylsuccinate for Oral Suspension USP, 200 mg/5 mL and 400 mg/5 mL contain the following inactive ingredients: lactose anhydrous, methylparaben, sodium citrate anhydrous, povidone, simethicone, cherry flavor, polysorbate 80, and sucrose.