
Metoprolol Succinate
These highlights do not include all the information needed to use metoprolol succinate extended-release tablets safely and effectively. See full prescribing information for metoprolol succinate extended-release tablets. METOPROLOL succinate extended-release tablets USP, for oral use Initial U.S. Approval: 1992
b195e7e8-f40c-4a49-a079-f1824b701325
HUMAN PRESCRIPTION DRUG LABEL
Sep 25, 2023
PD-Rx Pharmaceuticals, Inc.
DUNS: 156893695
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Metoprolol Succinate
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (10)
Drug Labeling Information
WARNINGS AND PRECAUTIONS SECTION
5 WARNINGS AND PRECAUTIONS
5.1 Ischemic Heart Disease
Following abrupt cessation of therapy with certain beta-blocking agents, exacerbations of angina pectoris and, in some cases, myocardial infarction have occurred. When discontinuing chronically administered metoprolol succinate extended-release tablets, particularly in patients with ischemic heart disease, gradually reduce the dosage over a period of 1 - 2 weeks and monitor the patient. If angina markedly worsens or acute coronary ischemia develops, promptly reinstate metoprolol succinate extended-release tablets, and take measures appropriate for the management of unstable angina. Warn patients not to interrupt therapy without their physician’s advice. Because coronary artery disease is common and may be unrecognized, avoid abruptly discontinuing metoprolol succinate extended-release tablets in patients treated only for hypertension.
5.2 Heart Failure
Worsening cardiac failure may occur during up-titration of metoprolol succinate extended-release tablets. If such symptoms occur, increase diuretics and restore clinical stability before advancing the dose of metoprolol succinate extended-release tablets [see Dosage and Administration (2)]. It may be necessary to lower the dose of metoprolol succinate extended-release tablets or temporarily discontinue it. Such episodes do not preclude subsequent successful titration of metoprolol succinate extended-release tablets.
5.3 Bronchospastic Disease
PATIENTS WITH BRONCHOSPASTIC DISEASES SHOULD, IN GENERAL, NOT RECEIVE BETA- BLOCKERS. Because of its relative beta 1 cardio-selectivity, however, metoprolol succinate extended-release tablets may be used in patients with bronchospastic disease who do not respond to, or cannot tolerate, other antihypertensive treatment. Because beta 1-selectivity is not absolute, use the lowest possible dose of metoprolol succinate extended-release tablets. Bronchodilators, including beta 2-agonists, should be readily available or administered concomitantly [see Dosage and Administration (2)].
5.4 Pheochromocytoma
If metoprolol succinate extended-release tablets are used in the setting of pheochromocytoma, it should be given in combination with an alpha blocker, and only after the alpha blocker has been initiated. Administration of beta- blockers alone in the setting of pheochromocytoma has been associated with a paradoxical increase in blood pressure due to the attenuation of beta-mediated vasodilatation in skeletal muscle.
5.5 Major Surgery
Avoid initiation of a high-dose regimen of extended-release metoprolol in patients undergoing non-cardiac surgery, since such use in patients with cardiovascular risk factors has been associated with bradycardia, hypotension, stroke and death.
Chronically administered beta-blocking therapy should not be routinely withdrawn prior to major surgery, however, the impaired ability of the heart to respond to reflex adrenergic stimuli may augment the risks of general anesthesia and surgical procedures.
5.6 Diabetes and Hypoglycemia
Beta-blockers may mask tachycardia occurring with hypoglycemia, but other manifestations such as dizziness and sweating may not be significantly affected.
5.7 Hepatic Impairment
Consider initiating metoprolol succinate extended-release tablets therapy at doses lower than those recommended for a given indication; gradually increase dosage to optimize therapy, while monitoring closely for adverse events.
5.8 Thyrotoxicosis
Beta-adrenergic blockade may mask certain clinical signs of hyperthyroidism, such as tachycardia. Abrupt withdrawal of beta-blockade may precipitate a thyroid storm.
5.9 Anaphylactic Reaction
While taking beta-blockers, patients with a history of severe anaphylactic reactions to a variety of allergens may be more reactive to repeated challenge and may be unresponsive to the usual doses of epinephrine used to treat an allergic reaction.
5.10 Peripheral Vascular Disease
Beta-blockers can precipitate or aggravate symptoms of arterial insufficiency in patients with peripheral vascular disease.
5.11 Calcium Channel Blockers
Because of significant inotropic and chronotropic effects in patients treated with beta-blockers and calcium channel blockers of the verapamil and diltiazem type, caution should be exercised in patients treated with these agents concomitantly.
- Heart Failure: Worsening cardiac failure may occur. ( 5.2)
- Bronchospastic Disease: Avoid beta blockers. ( 5.3)
- Pheochromocytoma: If required, first initiate therapy with an alpha blocker. ( 5.4)
- Major Surgery: Avoid initiation of high-dose extended-release metoprolol in patients undergoing non-cardiac surgery because it has been associated with bradycardia, hypotension, stroke and death. Do not routinely withdraw chronic beta blocker therapy prior to surgery. ( 5.5, 6.1)
- Diabetes and Hypoglycemia: May mask tachycardia occurring with hypoglycemia. ( 5.6)
- Patients with Hepatic Impairment: ( 5.7)
- Thyrotoxicosis: Abrupt withdrawal in patients with thyrotoxicosis might precipitate a thyroid storm. ( 5.8)
- Anaphylactic Reactions: Patients may be unresponsive to the usual doses of epinephrine used to treat allergic reaction. ( 5.9)
- Peripheral Vascular Disease: Can aggravate symptoms of arterial insufficiency. ( 5.10)
- Calcium Channel Blockers: Because of significant inotropic and chronotropic effects in patients treated with beta-blockers and calcium channel blockers of the verapamil and diltiazem type, caution should be exercised in patients treated with these agents concomitantly. ( 5.11)
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
7.1 Catecholamine Depleting Drugs
Catecholamine depleting drugs (eg, reserpine, monoamine oxidase (MAO) inhibitors) may have an additive effect when given with beta-blocking agents. Observe patients treated with metoprolol succinate extended-release tablets plus a catecholamine depletor for evidence of hypotension or marked bradycardia, which may produce vertigo, syncope, or postural hypotension.
7.2 CYP2D6 Inhibitors
Drugs that inhibit CYP2D6 such as quinidine, fluoxetine, paroxetine, and propafenone are likely to increase metoprolol concentration. In healthy subjects with CYP2D6 extensive metabolizer phenotype, coadministration of quinidine 100 mg and immediate-release metoprolol 200 mg tripled the concentration of S-metoprolol and doubled the metoprolol elimination half- life. In four patients with cardiovascular disease, coadministration of propafenone 150 mg t.i.d. with immediate-release metoprolol 50 mg t.i.d. resulted in two- to five-fold increases in the steady-state concentration of metoprolol. These increases in plasma concentration would decrease the cardioselectivity of metoprolol.
7.3 Digitalis, Clonidine, and Calcium Channel Blockers
Digitalis glycosides, clonidine, diltiazem and verapamil slow atrioventricular conduction and decrease heart rate. Concomitant use with beta blockers can increase the risk of bradycardia.
If clonidine and a beta blocker, such as metoprolol are coadministered, withdraw the beta-blocker several days before the gradual withdrawal of clonidine because beta-blockers may exacerbate the rebound hypertension that can follow the withdrawal of clonidine. If replacing clonidine by beta-blocker therapy, delay the introduction of beta-blockers for several days after clonidine administration has stopped [see Warnings and Precautions (5.11)].
- Catecholamine-depleting drugs may have an additive effect when given with beta-blocking agents. ( 7.1)
- CYP2D6 Inhibitors are likely to increase metoprolol concentration. ( 7.2)
- Concomitant use of glycosides, clonidine, and diltiazem and verapamil with beta-blockers can increase the risk of bradycardia. ( 7.3)
- Beta-blockers including metoprolol, may exacerbate the rebound hypertension that can follow the withdrawal of clonidine. ( 7.3)
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category C
Metoprolol tartrate has been shown to increase post-implantation loss and decrease neonatal survival in rats at doses up to 22 times, on a mg/m 2 basis, the daily dose of 200 mg in a 60-kg patient. Distribution studies in mice confirm exposure of the fetus when metoprolol tartrate is administered to the pregnant animal. These studies have revealed no evidence of impaired fertility or teratogenicity. There are no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, use this drug during pregnancy only if clearly needed.
8.3 Nursing Mothers
Metoprolol is excreted in breast milk in very small quantities. An infant consuming 1 liter of breast milk daily would receive a dose of less than 1 mg of the drug. Consider possible infant exposure when metoprolol succinate extended-release tablets are administered to a nursing woman.
8.4 Pediatric Use
One hundred forty-four hypertensive pediatric patients aged 6 to 16 years were randomized to placebo or to one of three dose levels of metoprolol succinate extended-release tablets (0.2, 1.0 or 2.0 mg/kg once daily) and followed for 4 weeks. The study did not meet its primary endpoint (dose response for reduction in SBP). Some pre-specified secondary endpoints demonstrated effectiveness including:
- Dose-response for reduction in DBP,
- mg/kg vs. placebo for change in SBP, and
- mg/kg vs. placebo for change in SBP and DBP.
The mean placebo corrected reductions in SBP ranged from 3 to 6 mmHg, and DBP from 1 to 5 mmHg. Mean reduction in heart rate ranged from 5 to 7 bpm but considerably greater reductions were seen in some individuals [see Dosage and Administration (2.1)].
No clinically relevant differences in the adverse event profile were observed for pediatric patients aged 6 to 16 years as compared with adult patients.
Safety and effectiveness of metoprolol succinate extended-release tablets have not been established in patients < 6 years of age.
8.5 Geriatric Use
Clinical studies of metoprolol succinate extended-release tablets in hypertension did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience in hypertensive patients has not identified differences in responses between elderly and younger patients.
Of the 1,990 patients with heart failure randomized to metoprolol succinate extended-release tablets in the MERIT-HF trial, 50% (990) were 65 years of age and older and 12% (238) were 75 years of age and older. There were no notable differences in efficacy or the rate of adverse reactions between older and younger patients.
In general, use a low initial starting dose in elderly patients given their greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
8.6 Hepatic Impairment
No studies have been performed with metoprolol succinate extended-release tablets in patients with hepatic impairment. Because metoprolol succinate extended-release tablets are metabolized by the liver, metoprolol blood levels are likely to increase substantially with poor hepatic function. Therefore, initiate therapy at doses lower than those recommended for a given indication; and increase doses gradually in patients with impaired hepatic function.
8.7 Renal Impairment
The systemic availability and half-life of metoprolol in patients with renal failure do not differ to a clinically significant degree from those in normal subjects. No reduction in dosage is needed in patients with chronic renal failure [see Clinical Pharmacology (12.3)].
- Pregnancy: There are no adequate and well-controlled studies in pregnant women. Use this drug during pregnancy only if clearly needed. ( 8.1)
- Nursing Mothers: Consider possible infant exposure. ( 8.3)
- Pediatrics: Safety and effectiveness have not been established in patients < 6 years of age. ( 8.4)
- Geriatrics: No notable difference in efficacy or safety vs. younger patients. ( 8.5)
- Hepatic Impairment: Consider initiating metoprolol succinate extended-release tablets therapy at low doses and gradually increase dosage to optimize therapy, while monitoring closely for adverse events. ( 8.6)
DESCRIPTION SECTION
11 DESCRIPTION
Metoprolol succinate extended-release tablets are beta 1-selective (cardioselective) adrenoceptor blocking agent, for oral administration, available as extended-release tablets. Metoprolol succinate extended-release tablets have been formulated to provide a controlled and predictable release of metoprolol for once-daily administration. The tablets comprise a multiple unit system containing metoprolol succinate in a multitude of controlled release pellets. Each pellet acts as a separate drug delivery unit and is designed to deliver metoprolol continuously over the dosage interval. The tablets contain 23.75, 47.5, 95 and 190 mg of metoprolol succinate equivalent to 25, 50, 100 and 200 mg of metoprolol tartrate, USP, respectively. Its chemical name is (±)1(isopropylamino)-3-[p-(2-methoxyethyl) phenoxy]-2-propanol succinate (2:1) (salt). Its structural formula is:
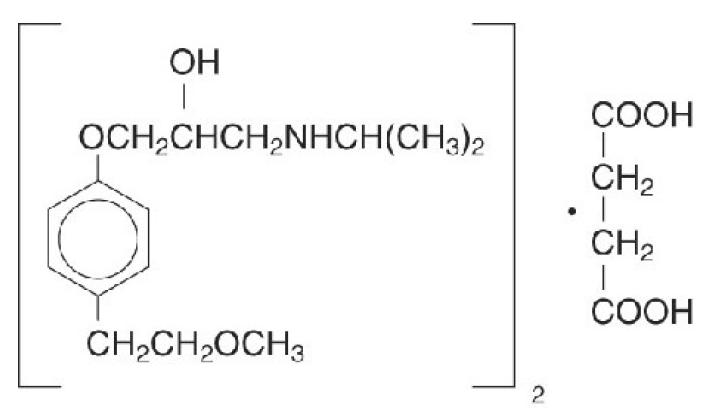
Metoprolol succinate is a white crystalline powder with a molecular weight of 652.8. It is freely soluble in water; soluble in methanol; sparingly soluble in ethanol; slightly soluble in dichloromethane and 2-propanol; practically insoluble in ethyl-acetate, acetone, diethylether and heptane. Inactive ingredients: ethyl cellulose, hypromellose type 2208, hypromellose type 2910, lecithin, magnesium stearate, microcrystalline cellulose, polyethylene glycol, talc, titanium dioxide.