
SEGLUROMET
These highlights do not include all the information needed to use SEGLUROMET safely and effectively. See full prescribing information for SEGLUROMET. SEGLUROMET (ertugliflozin and metformin hydrochloride) tablets, for oral use Initial U.S. Approval: 2017
9f720024-c68c-420c-aad7-c575237b6d39
HUMAN PRESCRIPTION DRUG LABEL
Nov 13, 2022
A-S Medication Solutions
DUNS: 830016429
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
ertugliflozin and metformin hydrochloride
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (12)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
ertugliflozin and metformin hydrochloride
BOXED WARNING SECTION
WARNING: LACTIC ACIDOSIS
See full prescribing information for complete boxed warning**.**
*Postmarketing cases of metformin-associated lactic acidosis have resulted in death, hypothermia, hypotension, and resistant bradyarrhythmias. Symptoms included malaise, myalgias, respiratory distress, somnolence, and abdominal pain. Laboratory abnormalities included elevated blood lactate levels, anion gap acidosis, increased lactate/pyruvate ratio, and metformin plasma levels generally >5 mcg/mL. (5.1) *Risk factors include renal impairment, concomitant use of certain drugs, age ≥65 years old, radiological studies with contrast, surgery and other procedures, hypoxic states, excessive alcohol intake, and hepatic impairment. Steps to reduce the risk of and manage metformin-associated lactic acidosis in these high risk groups are provided in the Full Prescribing Information. (5.1) *If lactic acidosis is suspected, discontinue SEGLUROMET and institute general supportive measures in a hospital setting. Prompt hemodialysis is recommended. (5.1)
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
SEGLUROMET® is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
Limitations of Use
Not recommended in patients with type 1 diabetes mellitus. It may increase the risk of diabetic ketoacidosis in these patients [see Warnings and Precautions (5.2)].
SEGLUROMET is a combination of ertugliflozin, a sodium glucose co-transporter 2 (SGLT2) inhibitor, and metformin, a biguanide, indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. (1)
Limitations of Use:
Not for the treatment of type 1 diabetes mellitus or diabetic ketoacidosis. It may increase the risk of diabetic ketoacidosis in these patients. (1)
CONTRAINDICATIONS SECTION
4 CONTRAINDICATIONS
- Hypersensitivity to ertugliflozin, metformin, or any excipient in SEGLUROMET, reactions such as angioedema or anaphylaxis have occurred [see Adverse Reactions (6.2)].
- Patients with severe renal impairment (eGFR less than 30 mL/min/1.73 m2), end stage-renal disease (ESRD), or on dialysis [see Use in Specific Populations (8.6)].
- Acute or chronic metabolic acidosis, including diabetic ketoacidosis, with or without coma.
- Severe renal impairment (eGFR less than 30 mL/min/1.73 m2), end stage-renal disease, or patients on dialysis. (4, 5.1, 5.2)
- Metabolic acidosis, including diabetic ketoacidosis. (4, 5.1)
- Hypersensitivity to ertugliflozin, metformin or any excipient. (4)
ADVERSE REACTIONS SECTION
6 ADVERSE REACTIONS
The following important adverse reactions are described elsewhere in the labeling:
- Lactic Acidosis [see Boxed Warning and Warnings and Precautions (5.1)]
- Ketoacidosis [see Warnings and Precautions (5.2)]
- Lower Limb Amputation [see Warnings and Precautions (5.3)]
- Volume Depletion [see Warnings and Precautions (5.4)]
- Urosepsis and Pyelonephritis [see Warnings and Precautions (5.5)]
- Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues [see Warnings and Precautions (5.6)]
- Necrotizing Fasciitis of the Perineum (Fournier's Gangrene) [see Warnings and Precautions (5.7)]
- Genital Mycotic Infections [see Warnings and Precautions (5.8)]
- Vitamin B12 Deficiency [see Warnings and Precautions (5.9)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Ertugliflozin and Metformin Hydrochloride
The incidence and type of adverse reactions in the two 26-week, placebo- controlled trials of ertugliflozin 5 mg and 15 mg added to metformin, representing a majority of data from the three 26-week, placebo-controlled trials, were similar to the adverse reactions described in Table 1.
Ertugliflozin
Pool of Placebo-Controlled Trials
The data in Table 1 are derived from a pool of three 26-week, placebo- controlled trials. Ertugliflozin was used as monotherapy in one trial and as add-on therapy in two trials [see Clinical Studies (14)]. These data reflect exposure of 1,029 patients to ertugliflozin with a mean exposure duration of approximately 25 weeks. Patients received ertugliflozin 5 mg (N=519), ertugliflozin 15 mg (N=510), or placebo (N=515) once daily. The mean age of the population was 57 years and 2% were older than 75 years of age. Fifty- three percent (53%) of the population was male and 73% were Caucasian, 15% were Asian, and 7% were Black or African American. At baseline the population had diabetes for an average of 7.5 years, had a mean HbA1c of 8.1%, and 19.4% had established microvascular complications of diabetes. Baseline renal function (mean eGFR 88.9 mL/min/1.73 m2) was normal or mildly impaired in 97% of patients and moderately impaired in 3% of patients.
Table 1 shows common adverse reactions associated with the use of ertugliflozin. These adverse reactions were not present at baseline, occurred more commonly on ertugliflozin than on placebo, and occurred in at least 2% of patients treated with either ertugliflozin 5 mg or ertugliflozin 15 mg.
Table 1: Adverse Reactions Reported in ≥2% of Patients with Type 2 Diabetes Mellitus Treated with Ertugliflozin* and Greater than Placebo in Pooled Placebo-Controlled Clinical Studies of Ertugliflozin Monotherapy or Combination Therapy|
Number (%) of Patients | |||
|---|---|---|---|
|
Placebo |
Ertugliflozin 5 mg |
Ertugliflozin 15 mg | |
Þ | |||
|
Female genital mycotic infections† |
3.0% |
9.1% |
12.2% |
|
Male genital mycotic infections‡ |
0.4% |
3.7% |
4.2% |
|
Urinary tract infections§ |
3.9% |
4.0% |
4.1% |
|
Headache |
2.3% |
3.5% |
2.9% |
|
Vaginal pruritus¶ |
0.4% |
2.8% |
2.4% |
|
Increased urination# |
1.0% |
2.7% |
2.4% |
|
Nasopharyngitis |
2.3% |
2.5% |
2.0% |
|
Back pain |
2.3% |
1.7% |
2.5% |
|
Weight decreased |
1.0% |
1.2% |
2.4% |
|
ThirstÞ |
0.6% |
2.7% |
1.4% |
Ketoacidosis
In a long-term cardiovascular outcomes study VERTIS CV (eValuation of ERTugliflozin effIcacy and Safety, CardioVascular [see Clinical Studies (14.2)], a study in patients with type 2 diabetes and established cardiovascular disease, ketoacidosis was identified in 19 (0.3%) ertugliflozin-treated patients and in 2 (0.1%) placebo-treated patients. Across seven other ertugliflozin clinical trials, ketoacidosis was identified in 3 (0.1%) ertugliflozin-treated patients and 0.0% of comparator-treated patients [see Warnings and Precautions (5.3)].
Volume Depletion
Ertugliflozin causes an osmotic diuresis, which may lead to intravascular volume contraction and adverse reactions related to volume depletion, particularly in patients with impaired renal function (eGFR less than 60 mL/min/1.73 m2). In patients with moderate renal impairment, adverse reactions related to volume depletion (e.g., dehydration, dizziness postural, presyncope, syncope, hypotension, and orthostatic hypotension) were reported in 0%, 4.4%, and 1.9% of patients treated with placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg, respectively. Ertugliflozin may also increase the risk of hypotension in other patients at risk for volume contraction [see Use in Specific Populations (8.5, 8.6)].
Hypoglycemia
The incidence of hypoglycemia by study is shown in Table 2.
Table 2: Incidence of Overall* and Severe† Hypoglycemia in Placebo- Controlled Clinical Studies in Patients with Type 2 Diabetes Mellitus
| |||
|
Add-on Combination Therapy with Metformin (26 weeks) |
Placebo |
Ertugliflozin |
Ertugliflozin |
|
Overall [N (%)] |
9 (4.3) |
15 (7.2) |
16 (7.8) |
|
Severe [N (%)] |
1 (0.5) |
1 (0.5) |
0 (0.0) |
|
Add-on Combination Therapy with Metformin and Sitagliptin (26 weeks) |
Placebo |
Ertugliflozin |
Ertugliflozin |
|
Overall [N (%)] |
5 (3.3) |
7 (4.5) |
3 (2.0) |
|
Severe [N (%)] |
1 (0.7) |
1 (0.6) |
0 (0.0) |
|
Add-on Combination with Insulin with or without Metformin (18 weeks) |
Placebo |
Ertugliflozin |
Ertugliflozin |
|
Overall [N (%)] |
130 (37.5) |
137 (39.4) |
144 (38.9) |
|
Severe [N (%)] |
12 (3.5) |
13 (3.7) |
19 (5.1) |
|
Add-on Combination with Metformin and a Sulfonylurea (18 weeks) |
Placebo |
Ertugliflozin |
Ertugliflozin |
|
Overall [N (%)] |
17 (14.5) |
20 (20.0) |
30 (26.5) |
|
Severe [N (%)] |
1 (0.9) |
2 (2.0) |
2 (1.8) |
Genital Mycotic Infections
In the pool of three placebo-controlled clinical trials, the incidence of female genital mycotic infections (e.g., genital candidiasis, genital infection fungal, vaginal infection, vulvitis, vulvovaginal candidiasis, vulvovaginal mycotic infection, vulvovaginitis) occurred in 3%, 9.1%, and 12.2%, of females treated with placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg, respectively (see Table 1). In females, discontinuation due to genital mycotic infections occurred in 0% and 0.6% of patients treated with placebo and ertugliflozin, respectively.
In the same pool, male genital mycotic infections (e.g., balanitis candida, balanoposthitis, genital infection, genital infection fungal) occurred in 0.4%, 3.7%, and 4.2% of males treated with placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg, respectively. Male genital mycotic infections occurred more commonly in uncircumcised males. In males, discontinuations due to genital mycotic infections occurred in 0% and 0.2% of patients treated with placebo and ertugliflozin, respectively. Phimosis was reported in 8 of 1,729 (0.5%) male ertugliflozin-treated patients, of which four required circumcision.
Urinary Tract Infections
In VERTIS CV urinary tract infections (e.g., urinary tract infection, cystitis, dysuria) occurred in 10.2%, 12.2% and 12.0% of patients treated with placebo, ertugliflozin 5 mg and ertugliflozin 15 mg, respectively. The incidences of serious urinary tract infections were 0.8%, 0.9% and 0.4% with placebo, ertugliflozin 5 mg and ertugliflozin 15 mg, respectively.
Metformin
The most common (5% or greater incidence) established adverse reactions due to initiation of metformin therapy are diarrhea, nausea, vomiting, flatulence, abdominal discomfort, indigestion, asthenia, and headache.
In controlled clinical trials of metformin of 29 weeks duration, a decrease to subnormal levels of previously normal serum vitamin B12 levels was observed in approximately 7% of patients.
Laboratory Tests
Ertugliflozin
Changes in Serum Creatinine and eGFR
Initiation of ertugliflozin causes an increase in serum creatinine and decrease in eGFR within weeks of starting therapy and then these changes stabilize. In a study of patients with moderate renal impairment, larger mean changes were observed. In a long-term cardiovascular outcomes trial, an initial increase in serum creatinine and a decrease in eGFR within weeks of starting therapy was observed (at Week 6 eGFR changes of -2.7, -3.8 and -0.4 mL/min/1.73 m2 in the ertugliflozin 5 mg, ertugliflozin 15 mg and placebo arms, respectively). The initial decline was followed by a recovery toward baseline to Week 52 (eGFR change from baseline of - 0.4, - 1.1 and - 0.2 mL/min/1.73 m2 in ertugliflozin 5 mg, ertugliflozin 15 mg, and placebo arms, respectively). Acute hemodynamic changes may play a role in the early renal function changes observed with ertugliflozin since they are reversed after treatment discontinuation.
Increases in Low-Density Lipoprotein Cholesterol (LDL-C)
In the pool of three placebo-controlled trials, dose-related increases in LDL-C were observed in patients treated with ertugliflozin. Mean percent changes from baseline to Week 26 in LDL-C relative to placebo were 2.6% and 5.4% with ertugliflozin 5 mg and ertugliflozin 15 mg, respectively. The range of mean baseline LDL-C was 96.6 to 97.7 mg/dL across treatment groups.
Increases in Hemoglobin
In the pool of three placebo-controlled trials, mean changes (percent changes) from baseline to Week 26 in hemoglobin were -0.21 g/dL (-1.4%) with placebo, 0.46 g/dL (3.5%) with ertugliflozin 5 mg, and 0.48 g/dL (3.5%) with ertugliflozin 15 mg. The range of mean baseline hemoglobin was 13.90 to 14.00 g/dL across treatment groups. At the end of treatment, 0.0%, 0.2%, and 0.4% of patients treated with placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg, respectively, had a hemoglobin increase greater than 2 g/dL and above the upper limit of normal.
Increases in Serum Phosphate
In the pool of three placebo-controlled trials, mean changes (percent changes) from baseline in serum phosphate were 0.04 mg/dL (1.9%) with placebo, 0.21 mg/dL (6.8%) with ertugliflozin 5 mg, and 0.26 mg/dL (8.5%) with ertugliflozin 15 mg. The range of mean baseline serum phosphate was 3.53 to 3.54 mg/dL across treatment groups. In a clinical trial of patients with moderate renal impairment, mean changes (mean percent changes) from baseline at Week 26 in serum phosphate were -0.01 mg/dL (0.8%) with placebo, 0.29 mg/dL (9.7%) with ertugliflozin 5 mg, and 0.24 mg/dL (7.8%) with ertugliflozin 15 mg.
6.2 Postmarketing Experience
Additional adverse reactions have been identified during post approval use. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Necrotizing fasciitis of the perineum (Fournier’s Gangrene)
- Angioedema
- Cholestatic, hepatocellular, and mixed hepatocellular liver injury have been reported with postmarketing use of metformin.
- Most common adverse reactions associated with ertugliflozin (incidence ≥5%) were female genital mycotic infections. (6.1)
- Most common adverse reactions associated with metformin (incidence ≥5%) were diarrhea, nausea, vomiting, flatulence, abdominal discomfort, indigestion, asthenia, and headache. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Merck Sharp & Dohme LLC at 1-877-888-4231 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
Table 3: Clinically Significant Drug Interactions with SEGLUROMET|
Carbonic Anhydrase Inhibitors | |
|---|---|
|
Clinical Impact: |
The risk of lactic acidosis may increase due to concomitant use of Topiramate or other carbonic anhydrase inhibitors (e.g., zonisamide, acetazolamide or dichlorphenamide) with metformin. These drugs frequently cause a decrease in serum bicarbonate and induce non-anion gap, hyperchloremic metabolic acidosis. |
|
Intervention: |
more frequent monitoring of these patients. |
|
Drugs that Reduce Metformin Clearance | |
|
Clinical Impact: |
The risk of lactic acidosis may increase due to concomitant use of drugs that interfere with common renal tubular transport systems involved in the renal elimination of metformin (e.g., organic cationic transporter-2 [OCT2] / multidrug and toxin extrusion [MATE] inhibitors such as ranolazine, vandetanib, dolutegravir, and cimetidine) which increase systemic exposure to metformin |
|
Intervention |
Consider the benefits and risks of concomitant use. |
|
Alcohol | |
|
Clinical Impact: |
Potentiate the effect of metformin on lactate metabolism. |
|
Intervention: |
Warn patients against excessive alcohol intake while receiving SEGLUROMET. |
|
Insulin and Insulin Secretagogues | |
|
Clinical Impact: |
The risk of hypoglycemia when ertugliflozin is used in combination with insulin and/or an insulin secretagogue. |
|
Intervention: |
A lower dose of insulin or insulin secretagogue may be required to minimize the risk of hypoglycemia when used in combination with SEGLUROMET. |
|
Drugs that Affect Glycemic Control | |
|
Clinical Impact: |
Certain drugs tend to produce hyperglycemia and may lead to loss of glycemic control. These drugs include the thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blocking drugs, and isoniazid. |
|
Intervention: |
When a patient is receiving SEGLUROMET along with such drugs, the patient should be closely observed to maintain adequate glycemic control. |
|
Lithium | |
|
Clinical Impact: |
Concomitant use of an SGLT2 inhibitor with lithium may decrease serum lithium concentrations. |
|
Intervention: |
Monitor serum lithium concentration more frequently during SEGLUROMET initiation and dosage changes. |
|
Positive Urine Glucose Test | |
|
Clinical Impact: |
SGLT2 inhibitors increase urinary glucose excretion and will lead to positive urine glucose tests. |
|
Intervention: |
Monitoring glycemic control with urine glucose tests is not recommended in patients taking SEGLUROMET. Use alternative methods to monitor glycemic control. |
|
Interference with 1,5-anhydroglucitol (1,5-AG) Assay | |
|
Clinical Impact: |
Measurements of 1,5-AG are unreliable in assessing glycemic control in patients taking SGLT2 inhibitors. |
|
Intervention: |
Monitoring glycemic control with 1,5-AG assay is not recommended. Use alternative methods to monitor glycemic control. |
- Carbonic Anhydrase Inhibitors: May increase risk of lactic acidosis. Consider more frequent monitoring. (7.2)
- Drugs that Reduce Metformin Clearance: May increase risk of lactic acidosis. Consider benefits and risks of concomitant use. (7.2)
- See full prescribing information for additional drug interactions and information on interference of SEGLUROMET with laboratory tests. (7)
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Prior to Initiation of SEGLUROMET
- Assess renal function prior to initiation of SEGLUROMET and as clinically indicated [see Warnings and Precautions (5.2)].
- In patients with volume depletion, correct this condition before initiating SEGLUROMET [see Warnings and Precautions (5.4), Use in Specific Populations (8.5, 8.6)].
2.2 Recommended Dosage
- Individualize the starting dose of SEGLUROMET, ertugliflozin and metformin hydrochloride (HCl), based on the patient’s current regimen, while not exceeding the maximum recommended daily dose of 15 mg ertugliflozin and 2,000 mg metformin HCl:
- In patients on metformin HCl, switch to SEGLUROMET tablets containing 2.5 mg ertugliflozin, with a similar total daily dose of metformin HCl.
- In patients on ertugliflozin, switch to SEGLUROMET tablets containing 500 mg metformin HCl, with a similar total daily dose of ertugliflozin.
- In patients already treated with ertugliflozin and metformin HCl, switch to SEGLUROMET tablets containing the same total daily dose of ertugliflozin and a similar daily dose of metformin HCl.
- Take SEGLUROMET twice daily with meals, with gradual dose escalation for those initiating metformin HCl to reduce the gastrointestinal side effects due to metformin [see Adverse Reactions (6.1)].
- Dosing may be adjusted based on effectiveness and tolerability.
- Use of SEGLUROMET is not recommended in patients with an eGFR less than 45 mL/min/1.73 m2.
- Use of SEGLUROMET is contraindicated in patients with severe renal impairment (eGFR less than 30 mL/min/1.73 m2), end stage-renal disease (ESRD), or on dialysis [see Contraindications (4)].
2.3 Discontinuation for Iodinated Contrast Imaging Procedures
Discontinue SEGLUROMET at the time of, or prior to, an iodinated contrast imaging procedure in patients with an eGFR less than 60 mL/min/1.73 m2; in patients with a history of liver disease, alcoholism or heart failure; or in patients who will be administered intra-arterial iodinated contrast. Re- evaluate eGFR 48 hours after the imaging procedure; restart SEGLUROMET if renal function is stable [see Warnings and Precautions (5.1)].
- Assess renal function prior to initiation and as clinically indicated. (2.1)
- Correct volume depletion before initiation (2.1)
- Individualize the starting dose based on the patient's current regimen. (2.2)
- Maximum recommended dose is 7.5 mg ertugliflozin/1,000 mg metformin twice daily. (2.2)
- Take twice daily with meals, with gradual dose escalation. (2.2)
- Do not use in patients with an estimated glomerular filtration rate (eGFR) below 30 mL/minute/1.73 m2.
- Use is not recommended in patients with an eGFR less than 45 mL/min/1.73 m2. (2.2)
- Use is contraindicated in patients with severe renal impairment (eGFR less than 30 mL/min/1.73 m2), end stage-renal disease (ESRD), or on dialysis. (2.2)
- SEGLUROMET may need to be discontinued at time of, or prior to, iodinated contrast imaging procedures. (2.3)
DOSAGE FORMS & STRENGTHS SECTION
3 DOSAGE FORMS AND STRENGTHS
- Tablets: ertugliflozin 2.5 mg and metformin HCl 500 mg, pink, oval, debossed with "2.5/500" on one side and plain on the other side.
- Tablets: ertugliflozin 2.5 mg and metformin HCl 1,000 mg, pink, oval, debossed with "2.5/1000" on one side and plain on the other side.
- Tablets: ertugliflozin 7.5 mg and metformin HCl 500 mg, red, oval, debossed with "7.5/500" on one side and plain on the other side.
- Tablets: ertugliflozin 7.5 mg and metformin HCl 1,000 mg, red, oval, debossed with "7.5/1000" on one side and plain on the other side.
Tablets:
- Ertugliflozin 2.5 mg and metformin hydrochloride 500 mg (3)
- Ertugliflozin 2.5 mg and metformin hydrochloride 1,000 mg (3)
- Ertugliflozin 7.5 mg and metformin hydrochloride 500 mg (3)
- Ertugliflozin 7.5 mg and metformin hydrochloride 1,000 mg (3)
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on animal data showing adverse renal effects, from ertugliflozin, SEGLUROMET is not recommended during the second and third trimesters of pregnancy. Published studies with metformin use during pregnancy have not reported a clear association with metformin and major birth defect or miscarriage risk (see Data).
The limited available data with SEGLUROMET in pregnant women are not sufficient to determine a drug-associated risk for major birth defects or miscarriage. There are risks to the mother and fetus associated with poorly controlled diabetes in pregnancy (see Clinical Considerations).
In animal studies, adverse renal changes were observed in rats when ertugliflozin was administered during a period of renal development corresponding to the late second and third trimesters of human pregnancy. Doses approximately 13 times the maximum clinical dose caused renal pelvic and tubule dilatations and renal mineralization that were not fully reversible. There was no evidence of fetal harm in rats or rabbits at exposures of ertugliflozin approximately 300 times higher than the maximal clinical dose of 15 mg/day when administered during organogenesis (see Data).
The estimated background risk of major birth defects is 6-10% in women with pre-gestational diabetes with a HbA1c >7 and has been reported to be as high as 20-25% in women with HbA1c >10. The estimated background risk of miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
Poorly-controlled diabetes in pregnancy increases the maternal risk for diabetic ketoacidosis, pre-eclampsia, spontaneous abortions, preterm delivery, and delivery complications. Poorly controlled diabetes increases the fetal risk for major birth defects, stillbirth, and macrosomia related morbidity.
Data
Human Data
Published data from postmarketing studies have not reported a clear association with metformin and major birth defects, miscarriage, or adverse maternal or fetal outcomes when metformin was used during pregnancy. However, these studies cannot definitely establish the absence of any metformin- associated risk because of methodological limitations, including small sample size and inconsistent comparator groups.
Animal Data
Ertugliflozin
When ertugliflozin was orally administered to juvenile rats from PND 21 to PND 90, increased kidney weight, renal tubule and renal pelvis dilatation, and renal mineralization occurred at doses greater than or equal to 5 mg/kg (13-fold human exposures, based on AUC). These effects occurred with drug exposure during periods of renal development in rats that correspond to the late second and third trimester of human renal development, and did not fully reverse within a 1-month recovery period.
In embryo-fetal development studies, ertugliflozin (50, 100 and 250 mg/kg/day) was administered orally to rats on gestation days 6 to 17 and to rabbits on gestation days 7 to 19. Ertugliflozin did not adversely affect developmental outcomes in rats and rabbits at maternal exposures that were approximately 300 times the human exposure at the maximum clinical dose of 15 mg/day, based on AUC. A maternally toxic dose (250 mg/kg/day) in rats (707 times the clinical dose) was associated with reduced fetal viability and a higher incidence of a visceral malformation (membranous ventricular septal defect). In the pre- and post-natal development study in pregnant rats, ertugliflozin was administered to the dams from gestation day 6 through lactation day 21 (weaning). Decreased post-natal growth (weight gain) was observed at maternal doses ≥100 mg/kg/day (greater than or equal to 331 times the human exposure at the maximum clinical dose of 15 mg/day, based on AUC).
Metformin HCl
Metformin did not adversely affect development outcomes when administered to rats and rabbits at doses up to 600 mg/kg/day. This represents an exposure of about 2 and 6 times the maximum recommended human dose of 2,000 mg based on body surface area comparisons for rats and rabbits, respectively. Determination of fetal concentrations demonstrated a partial placental barrier to metformin.
8.2 Lactation
Risk Summary
There is no information regarding the presence of SEGLUROMET or ertugliflozin in human milk, the effects on the breastfed infant, or the effects on milk production. Limited published studies report that metformin is present in human milk (see Data). However, there is insufficient information on the effects of metformin on the breastfed infant and no available information on the effects of metformin on milk production. Ertugliflozin (see Data) and metformin are present in the milk of lactating rats. Since human kidney maturation occurs in utero and during the first 2 years of life when lactational exposure may occur, there may be risk to the developing human kidney, based on data with ertugliflozin. Because of the potential for serious adverse reactions in a breastfed infant, advise women that the use of SEGLUROMET is not recommended while breastfeeding.
Data
The lacteal excretion of radiolabeled ertugliflozin in lactating rats was evaluated 10 to 12 days after parturition. Ertugliflozin derived radioactivity exposure in milk and plasma were similar, with a milk/plasma ratio of 1.07, based on AUC. Juvenile rats directly exposed to ertugliflozin during a developmental period corresponding to human kidney maturation were associated with a risk to the developing kidney (persistent increased organ weight, renal mineralization, and renal pelvic and tubular dilatations).
Published clinical lactation studies report that metformin is present in human milk, which resulted in infant doses approximately 0.11% to 1% of the maternal weight-adjusted dosage and a milk/plasma ratio ranging between 0.13 and 1. However, the studies were not designed to definitely establish the risk of use of metformin during lactation because of small sample size and limited adverse event data collected in infants.
8.3 Females and Males of Reproductive Potential
Discuss the potential for unintended pregnancy with premenopausal women as therapy with metformin may result in ovulation in some anovulatory women.
8.4 Pediatric Use
Safety and effectiveness of SEGLUROMET in pediatric patients under 18 years of age have not been established.
8.5 Geriatric Use
SEGLUROMET
No dosage adjustment of SEGLUROMET is recommended based on age. Elderly patients are more likely to have decreased renal function. Because renal function abnormalities can occur after initiating ertugliflozin, and metformin is known to be substantially excreted by the kidneys, care should be taken in dose selection in the elderly. Assess renal function in elderly patients prior to initiating dosing and periodically thereafter [see Dosage and Administration (2.1) and Warnings and Precautions (5.1, 5.4)].
Ertugliflozin
In ertugliflozin clinical trials, a total of 876 (25.7%) patients treated with ertugliflozin were 65 years and older, and 152 (4.5%) patients treated with ertugliflozin were 75 years and older. Patients 65 years and older had a higher incidence of adverse reactions related to volume depletion compared to younger patients; events were reported in 1.1%, 2.2%, and 2.6% of patients treated with comparator, ertugliflozin 5 mg, and ertugliflozin 15 mg, respectively [see Warnings and Precautions (5.4) and Adverse Reactions (6.1)].
In VERTIS CV, a total of 2780 (50.5%) patients treated with ertugliflozin were 65 years and older, and 595 (10.8%) patients treated with ertugliflozin were 75 years and older. Safety and efficacy were generally similar for patients age 65 years and older compared to patients younger than 65.
Metformin HCl
Controlled clinical studies of metformin did not include sufficient numbers of elderly patients to determine whether they respond differently from younger patients, although other reported clinical experience has not identified differences in responses between the elderly and young patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy and the higher risk of lactic acidosis. Assess renal function more frequently in elderly patients [see Contraindications (4), Warnings and Precautions (5.1), and Clinical Pharmacology (12.3)].
8.6 Renal Impairment
A 26-week placebo-controlled study of 313 patients with Stage 3 Chronic Kidney Disease (eGFR ≥30 to less than 60 mL/min/1.73 m2) treated with ertugliflozin did not have improvement in glycemic control.
In the VERTIS CV study, there were 1370 patients (25%) with an eGFR ≥90 mL/min/1.73 m2, 2929 patients (53%) with an eGFR of ≥60 to less than 90 mL/min/1.73 m2, 879 patients (16%) with an eGFR of ≥45 to less than 60 mL/min/1.73 m2, and 299 patients (5%) with eGFR of 30 to <45 mL/min/1.73 m2 treated with ertugliflozin. Similar effects on glycemic control at Week 18 were observed in patients treated with ertugliflozin in each eGFR subgroup and also in the overall patient population.
SEGLUROMET is contraindicated in patients with severe renal impairment (eGFR less than 30 mL/min/1.73 m2), ESRD, or on dialysis [see Contraindications (4)].
No dosage adjustment is needed in patients with eGFR ≥45 mL/min/1.73 m2.
Metformin is substantially excreted by the kidney, and the risk of metformin accumulation and lactic acidosis increases with the degree of renal impairment.
8.7 Hepatic Impairment
Use of metformin in patients with hepatic impairment has been associated with some cases of lactic acidosis. SEGLUROMET is not recommended in patients with hepatic impairment [see Warnings and Precautions (5.1)].
- Pregnancy: Advise females of the potential risk to a fetus, especially during the second and third trimesters. (8.1)
- Lactation: Breastfeeding not recommended. (8.2)
- Females and Males of Reproductive Potential: Advise premenopausal females of the potential for an unintended pregnancy. (8.3)
- Geriatrics: Higher incidence of adverse reactions related to reduced intravascular volume. (5.3, 8.5)
- Renal impairment: Higher incidence of adverse reactions related to reduced intravascular volume and renal function. (5.3, 8.6)
- Hepatic impairment: Avoid use in patients with hepatic impairment. (8.7)
OVERDOSAGE SECTION
10 OVERDOSAGE
SEGLUROMET
In the event of an overdose with SEGLUROMET, contact the Poison Control Center. Employ the usual supportive measures as dictated by the patient's clinical status.
Ertugliflozin
Removal of ertugliflozin by hemodialysis has not been studied.
Metformin HCl
Overdose of metformin hydrochloride has occurred, including ingestion of amounts greater than 50 g (25 times the maximum recommended daily dose). Hypoglycemia was reported in approximately 10% of cases, but no causal association with metformin hydrochloride has been established. Lactic acidosis has been reported in approximately 32% of metformin overdose cases [see Warnings and Precautions (5.1)]. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
DESCRIPTION SECTION
11 DESCRIPTION
SEGLUROMET (ertugliflozin and metformin hydrochloride) tablet for oral use contains ertugliflozin L-pyroglutamic acid, a SGLT2 inhibitor, and metformin HCl, a member of the biguanide class.
Ertugliflozin
The chemical name of ertugliflozin L-pyroglutamic acid is (1S,2S,3S,4R,5S)-5-(4-chloro-3-(4-ethoxybenzyl)phenyl)-1-(hydroxymethyl)-6,8-dioxabicyclo[3.2.1]octane-2,3,4-triol, compound with (2S)-5-oxopyrrolidine-2-carboxylic acid. The molecular formula is C27H32ClNO10 and the molecular weight is 566.00.
The chemical structure is:
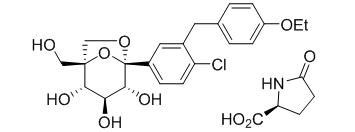
Ertugliflozin L-pyroglutamic acid is a white to off-white powder that is soluble in ethyl alcohol and acetone, slightly soluble in ethyl acetate and acetonitrile and very slightly soluble in water.
Metformin HCl
Metformin hydrochloride (N,N-dimethylimidodicarbonimidic diamide hydrochloride) is not chemically or pharmacologically related to any other classes of oral antihyperglycemic agents. The structural formula is as shown:
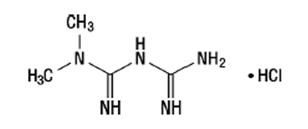
Metformin HCl is a white to off-white crystalline compound with a molecular formula of C4H11N5∙HCl and a molecular weight of 165.63. Metformin hydrochloride is freely soluble in water and is practically insoluble in acetone, ether and chloroform. The pKa of metformin is 12.4. The pH of a 1% aqueous solution of metformin hydrochloride is 6.68.
SEGLUROMET is available as film-coated tablets containing:
- 3.24 mg ertugliflozin L-pyroglutamic acid equivalent to 2.5 mg of ertugliflozin and 500 mg metformin HCl (SEGLUROMET 2.5/500)
- 3.24 mg ertugliflozin L-pyroglutamic acid equivalent to 2.5 mg of ertugliflozin and 1,000 mg metformin HCl (SEGLUROMET 2.5/1000)
- 9.71 mg ertugliflozin L-pyroglutamic acid equivalent to 7.5 mg of ertugliflozin and 500 mg metformin HCl (SEGLUROMET 7.5/500)
- 9.71 mg ertugliflozin L-pyroglutamic acid equivalent to 7.5 mg of ertugliflozin and 1,000 mg metformin HCl (SEGLUROMET 7.5/1000)
Inactive ingredients are povidone, microcrystalline cellulose, crospovidone, sodium lauryl sulfate, and magnesium stearate.
The film coating contains: hypromellose, hydroxypropyl cellulose, titanium dioxide, iron oxide red, and carnauba wax.
CLINICAL PHARMACOLOGY SECTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
SEGLUROMET
SEGLUROMET combines two antihyperglycemic agents with complementary mechanisms of action to improve glycemic control in patients with type 2 diabetes mellitus: ertugliflozin, a SGLT2 inhibitor, and metformin hydrochloride, a member of the biguanide class.
Ertugliflozin
SGLT2 is the predominant transporter responsible for reabsorption of glucose from the glomerular filtrate back into the circulation. Ertugliflozin is an inhibitor of SGLT2. By inhibiting SGLT2, ertugliflozin reduces renal reabsorption of filtered glucose and lowers the renal threshold for glucose, and thereby increases urinary glucose excretion.
Metformin HCl
Metformin is an antihyperglycemic agent which improves glucose tolerance in patients with type 2 diabetes mellitus, lowering both basal and postprandial plasma glucose. Its pharmacologic mechanisms of action are different from other classes of oral antihyperglycemic agents. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. Metformin does not produce hypoglycemia in either patients with type 2 diabetes mellitus or normal subjects (except in special circumstances) [see Warnings and Precautions (5.5)] and does not cause hyperinsulinemia. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and day-long plasma insulin response may actually decrease.
12.2 Pharmacodynamics
Ertugliflozin
Urinary Glucose Excretion and Urinary Volume
Dose-dependent increases in the amount of glucose excreted in urine were observed in healthy subjects and in patients with type 2 diabetes mellitus following single- and multiple-dose administration of ertugliflozin. Dose- response modeling indicates that ertugliflozin 5 mg and 15 mg result in near maximal urinary glucose excretion (UGE). Enhanced UGE is maintained after multiple-dose administration. UGE with ertugliflozin also results in increases in urinary volume.
Cardiac Electrophysiology
The effect of ertugliflozin on QTc interval was evaluated in a Phase 1 randomized, placebo- and positive-controlled 3-period crossover study in 42 healthy subjects. At 6.7 times the therapeutic exposures with maximum recommended dose, ertugliflozin does not prolong QTc to any clinically relevant extent.
12.3 Pharmacokinetics
General Introduction
Ertugliflozin
The pharmacokinetics of ertugliflozin are similar in healthy subjects and patients with type 2 diabetes mellitus. The steady state mean plasma AUC and Cmax were 398 ng∙hr/mL and 81.3 ng/mL, respectively, with 5 mg ertugliflozin once-daily treatment, and 1,193 ng∙hr/mL and 268 ng/mL, respectively, with 15 mg ertugliflozin once-daily treatment. Steady-state is reached after 4 to 6 days of once-daily dosing with ertugliflozin. Ertugliflozin does not exhibit time-dependent pharmacokinetics and accumulates in plasma up to 10-40% following multiple dosing.
Absorption
SEGLUROMET
The effects of a high-fat meal on the pharmacokinetics of ertugliflozin and metformin when administered as SEGLUROMET tablets are comparable to those reported for the individual tablets. Food had no meaningful effect on AUCinf of ertugliflozin and metformin, but reduced mean ertugliflozin Cmax by approximately 41% and metformin Cmax by approximately 29% compared to the fasted condition.
Ertugliflozin
Following single-dose oral administration of 5 mg and 15 mg of ertugliflozin, peak plasma concentrations of ertugliflozin occur at 1 hour postdose (median Tmax) under fasted conditions. Plasma Cmax and AUC of ertugliflozin increase in a dose-proportional manner following single doses from 0.5 mg (0.1 times the lowest recommended dose) to 300 mg (20 times the highest recommended dose) and following multiple doses from 1 mg (0.2 times the lowest recommended dose) to 100 mg (6.7 times the highest recommended dose). The absolute oral bioavailability of ertugliflozin following administration of a 15 mg dose is approximately 100%.
Effect of Food
Administration of ertugliflozin with a high-fat and high-calorie meal decreases ertugliflozin Cmax by 29% and prolongs Tmax by 1 hour, but does not alter AUC as compared with the fasted state. The observed effect of food on ertugliflozin pharmacokinetics is not considered clinically relevant, and ertugliflozin may be administered with or without food. In Phase 3 clinical trials, ertugliflozin was administered without regard to meals.
Metformin hydrochloride
The absolute bioavailability of a metformin HCl 500-mg tablet given under fasting conditions is approximately 50-60%. Studies using single oral doses of metformin hydrochloride tablets 500 mg to 1,500 mg, and 850 mg to 2,550 mg (approximately 1.3 times the maximum recommended daily dosage), indicate that there is a lack of dose proportionality with increasing doses, which is due to decreased absorption rather than an alternation in elimination. Food decreases the extent of and slightly delays the absorption of metformin, as shown by approximately a 40% lower mean peak plasma concentration (Cmax), a 25% lower area under the plasma concentration versus time curve (AUC), and a 35-minute prolongation of time to peak plasma concentration (Tmax) following administration of a single 850-mg tablet of metformin with food, compared to the same tablet strength administered fasting. The clinical relevance of these decreases is unknown.
Distribution
Ertugliflozin
The mean steady-state volume of distribution of ertugliflozin following an intravenous dose is 85.5 L. Plasma protein binding of ertugliflozin is 93.6% and is independent of ertugliflozin plasma concentrations. Plasma protein binding is not meaningfully altered in patients with renal or hepatic impairment. The blood-to-plasma concentration ratio of ertugliflozin is 0.66.
Metformin
The apparent volume of distribution (V/F) of metformin following single oral doses of metformin hydrochloride tablets 850 mg averaged 654 ± 358 L. Metformin is negligibly bound to plasma proteins, in contrast to sulfonylureas, which are more than 90% protein bound. Metformin partitions into erythrocytes, most likely as a function of time. At usual clinical doses and dosing schedules of metformin hydrochloride tablets, steady-state plasma concentrations of metformin are reached within 24-48 hours and are generally <1 mcg/mL. During controlled clinical trials of metformin, maximum metformin plasma levels did not exceed 5 mcg/mL, even at maximum doses.
Elimination
Metabolism
Ertugliflozin
Metabolism is the primary clearance mechanism for ertugliflozin. The major metabolic pathway for ertugliflozin is UGT1A9 and UGT2B7-mediated O-glucuronidation to two glucuronides that are pharmacologically inactive at clinically relevant concentrations. CYP-mediated (oxidative) metabolism of ertugliflozin is minimal (12%).
Metformin
Intravenous single-dose studies in normal subjects demonstrate that metformin is excreted unchanged in the urine and does not undergo hepatic metabolism (no metabolites have been identified in humans) nor biliary excretion.
Excretion
Ertugliflozin
The mean systemic plasma clearance following an intravenous 100 µg dose was 11.2 L/hr. The mean elimination half-life in type 2 diabetic patients with normal renal function was estimated to be 16.6 hours based on the population pharmacokinetic analysis. Following administration of an oral [14C]-ertugliflozin solution to healthy subjects, approximately 40.9% and 50.2% of the drug-related radioactivity was eliminated in feces and urine, respectively. Only 1.5% of the administered dose was excreted as unchanged ertugliflozin in urine and 33.8% as unchanged ertugliflozin in feces, which is likely due to biliary excretion of glucuronide metabolites and subsequent hydrolysis to parent.
Metformin
Renal clearance is approximately 3.5 times greater than creatinine clearance, which indicates that tubular secretion is the major route of metformin elimination. Following oral administration, approximately 90% of the absorbed drug is eliminated via the renal route within the first 24 hours, with a plasma elimination half-life of approximately 6.2 hours. In blood, the elimination half-life is approximately 17.6 hours, suggesting that the erythrocyte mass may be a compartment of distribution.
Specific Populations
Patients with Renal Impairment
SEGLUROMET
Studies characterizing the pharmacokinetics of ertugliflozin and metformin after administration of SEGLUROMET in renally impaired patients have not been performed [see Dosage and Administration (2.2)].
Ertugliflozin
In a clinical pharmacology study in patients with type 2 diabetes mellitus and mild, moderate, or severe renal impairment (as determined by eGFR), following a single-dose administration of 15 mg ertugliflozin, the mean increases in AUC of ertugliflozin were 1.6-, 1.7-, and 1.6-fold, respectively, for mild, moderate, and severe renally-impaired patients compared to subjects with normal renal function. These increases in ertugliflozin AUC are not considered clinically meaningful. The 24-hour urinary glucose excretion declined with increasing severity of renal impairment [see Warnings and Precautions (5.2) and Use in Specific Populations (8.6)]. The plasma protein binding of ertugliflozin was unaffected in patients with renal impairment.
Metformin
In patients with decreased renal function, the plasma and blood half-life of metformin is prolonged and the renal clearance is decreased [see Contraindications (4) and Warnings and Precautions (5.1)].
Patients with Hepatic Impairment
Ertugliflozin
Moderate hepatic impairment (based on the Child-Pugh classification) did not result in an increase in exposure of ertugliflozin. The AUC of ertugliflozin decreased by approximately 13%, and Cmax decreased by approximately 21% compared to subjects with normal hepatic function. This decrease in ertugliflozin exposure is not considered clinically meaningful. There is no clinical experience in patients with Child-Pugh class C (severe) hepatic impairment. The plasma protein binding of ertugliflozin was unaffected in patients with moderate hepatic impairment [see Use in Specific Populations (8.7)].
Metformin
No pharmacokinetic studies of metformin have been conducted in patients with hepatic impairment [see Use in Specific Populations (8.7)].
Effects of Age, Body Weight, Gender, and Race
Ertugliflozin
Based on a population pharmacokinetic analysis, age, body weight, gender, and race do not have a clinically meaningful effect on the pharmacokinetics of ertugliflozin.
Metformin
Limited data from controlled pharmacokinetic studies of metformin in healthy elderly subjects suggest that total plasma clearance of metformin is decreased, the half-life is prolonged, and Cmax is increased, compared to healthy young subjects. From these data, it appears that the change in metformin pharmacokinetics with aging is primarily accounted for by a change in renal function.
Metformin pharmacokinetic parameters did not differ significantly between normal subjects and patients with type 2 diabetes mellitus when analyzed according to gender. Similarly, in controlled clinical studies in patients with type 2 diabetes mellitus, the antihyperglycemic effect of metformin was comparable in males and females.
No studies of metformin pharmacokinetic parameters according to race have been performed. In controlled clinical studies of metformin in patients with type 2 diabetes mellitus, the antihyperglycemic effect was comparable in Whites (n=249), Blacks (n=51), and Hispanics (n=24).
Drug Interaction Studies
SEGLUROMET
Coadministration of single dose of ertugliflozin (15 mg) and metformin (1,000 mg) did not meaningfully alter the pharmacokinetics of either ertugliflozin or metformin in healthy subjects.
Pharmacokinetic drug interaction studies with SEGLUROMET have not been performed; however, such studies have been conducted with ertugliflozin and metformin, the individual components of SEGLUROMET.
Ertugliflozin
In Vitro Assessment of Drug Interactions
In in vitro studies, ertugliflozin and ertugliflozin glucuronides did not inhibit CYP450 isoenzymes (CYPs) 1A2, 2C9, 2C19, 2C8, 2B6, 2D6, or 3A4, and did not induce CYPs 1A2, 2B6, or 3A4. Ertugliflozin was not a time-dependent inhibitor of CYP3A in vitro. Ertugliflozin did not inhibit UGT1A6, 1A9, or 2B7 in vitro and was a weak inhibitor (IC50 >39 µM) of UGT1A1 and 1A4. Ertugliflozin glucuronides did not inhibit UGT1A1, 1A4, 1A6, 1A9, or 2B7 in vitro. Overall, ertugliflozin is unlikely to affect the pharmacokinetics of drugs eliminated by these enzymes. Ertugliflozin is a substrate of P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP) transporters and is not a substrate of organic anion transporters (OAT1, OAT3), organic cation transporters (OCT1, OCT2), or organic anion transporting polypeptides (OATP1B1, OATP1B3). Ertugliflozin or ertugliflozin glucuronides do not meaningfully inhibit P-gp, OCT2, OAT1, or OAT3 transporters, or transporting polypeptides OATP1B1 and OATP1B3, at clinically relevant concentrations. Overall, ertugliflozin is unlikely to affect the pharmacokinetics of concurrently administered medications that are substrates of these transporters.
In Vivo Assessment of Drug Interactions
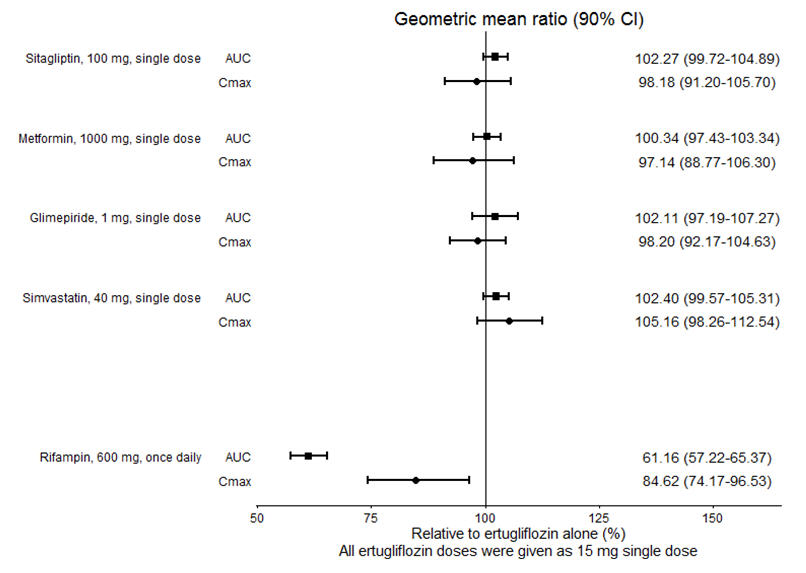
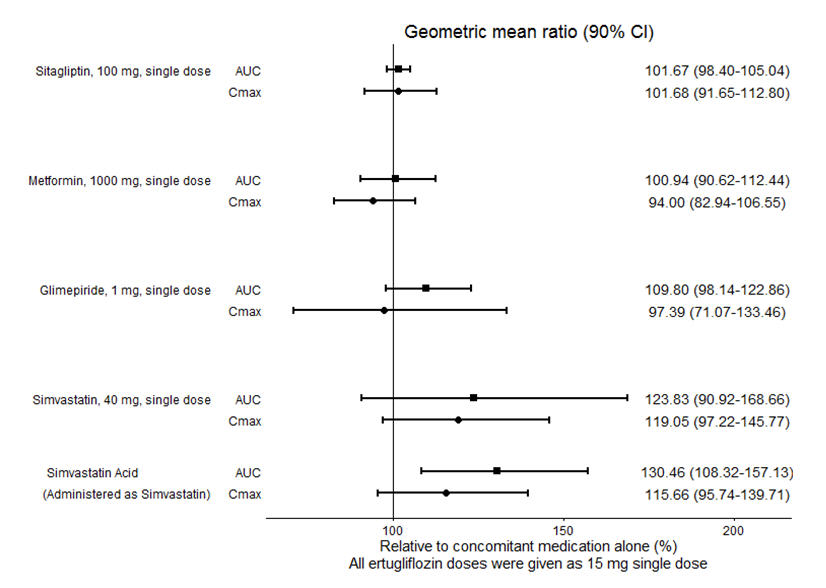
No dose adjustment of SEGLUROMET is recommended when coadministered with commonly prescribed medicinal products. Ertugliflozin pharmacokinetics were similar with and without coadministration of metformin, glimepiride, sitagliptin, and simvastatin in healthy subjects (see Figure 1). Coadministration of ertugliflozin with multiple doses of 600 mg once-daily rifampin (an inducer of UGT and CYP enzymes) resulted in approximately 39% and 15% mean reductions in ertugliflozin AUC and Cmax, respectively, relative to ertugliflozin administered alone. These changes in exposure are not considered clinically relevant. Ertugliflozin had no clinically relevant effect on the pharmacokinetics of metformin, glimepiride, sitagliptin, and simvastatin when coadministered in healthy subjects (see Figure 2). Physiologically-based PK (PBPK) modeling suggests that coadministration of mefenamic acid (UGT inhibitor) may increase the AUC and Cmax of ertugliflozin by 1.51- and 1.19-fold, respectively. These predicted changes in exposure are not considered clinically relevant.
Figure 1: Effects of Other Drugs on the Pharmacokinetics of Ertugliflozin|
|
|
|
Metformin hydrochloride
Table 4: Effect of Metformin HCl on Systemic Exposure of Coadministered Drugs|
Coadministered Drug |
Dose of Coadministered Drug* |
Dose of Metformin HCl* |
Geometric Mean Ratio | ||
|---|---|---|---|---|---|
|
AUC† |
Cmax | ||||
|
No dosing adjustments required for the following: | |||||
| |||||
|
Cimetidine |
400 mg |
850 mg |
Cimetidine |
0.95‡ |
1.01 |
|
Glyburide |
5 mg |
500 mg§ |
Glyburide |
0.78¶ |
0.63¶ |
|
Furosemide |
40 mg |
850 mg |
Furosemide |
0.87¶ |
0.69¶ |
|
Nifedipine |
10 mg |
850 mg |
Nifedipine |
1.10‡ |
1.08 |
|
Propranolol |
40 mg |
850 mg |
Propranolol |
1.01‡ |
0.94 |
|
Ibuprofen |
400 mg |
850 mg |
Ibuprofen |
0.97# |
1.01# |
|
Coadministered Drug |
Dose of Coadministered Drug* |
Dose of Metformin HCl* |
Geometric Mean Ratio | ||
|---|---|---|---|---|---|
|
AUC† |
Cmax | ||||
| |||||
|
No dosing adjustments required for the following: | |||||
|
Glyburide |
5 mg |
500 mg‡ |
Metformin‡ |
0.98§ |
0.99§ |
|
Furosemide |
40 mg |
850 mg |
Metformin |
1.09§ |
1.22§ |
|
Nifedipine |
10 mg |
850 mg |
Metformin |
1.16 |
1.21 |
|
Propranolol |
40 mg |
850 mg |
Metformin |
0.90 |
0.94 |
|
Ibuprofen |
400 mg |
850 mg |
Metformin |
1.05§ |
1.07§ |
|
Drugs that are eliminated by renal tubular secretion may increase the accumulation of metformin** [see**** Warnings and Precautions (5.1) and Drug Interactions (7.2)****].** | |||||
|
Cimetidine |
400 mg |
850 mg |
Metformin |
1.40 |
1.61 |
|
Carbonic anhydrase inhibitors may cause metabolic acidosis** [see**** Warnings and Precautions (5.1)and Drug Interactions (7.2)****].** | |||||
|
Topiramate |
100 mg¶ |
500 mg¶ |
Metformin |
1.25¶ |
1.17 |
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Ertugliflozin
Carcinogenicity was evaluated in CD-1 mice and Sprague-Dawley rats. In the mouse study, ertugliflozin was administered by oral gavage at doses of 5, 15, and 40 mg/kg/day for up to 97 weeks in males and 102 weeks in females. There were no ertugliflozin-related neoplastic findings at doses up to 40 mg/kg/day (approximately 50 times human exposure at the maximum recommended human dose [MRHD] of 15 mg/day based on AUC). In the rat study, ertugliflozin was administered by oral gavage at doses of 1.5, 5, and 15 mg/kg/day for up to 92 weeks in females and 104 weeks in males. Ertugliflozin-related neoplastic findings included an increased incidence of adrenal medullary pheochromocytoma (PCC) in male rats at 15 mg/kg/day. Although the molecular mechanism remains unknown, this finding may be related to carbohydrate malabsorption leading to altered calcium homeostasis, which has been associated with PCC development in rats and has unclear relevancy to human risk. The no-observed-effect level (NOEL) for neoplasia was 5 mg/kg/day (approximately 16 times human exposure at the MRHD of 15 mg/day, based on AUC).
Metformin HCl
Long-term carcinogenicity studies have been performed in rats (dosing duration of 104 weeks) and mice (dosing duration of 91 weeks) at doses up to and including 900 mg/kg/day and 1,500 mg/kg/day, respectively. These doses are both approximately four times the maximum recommended human daily dose of 2,000 mg based on body surface area comparisons. No evidence of carcinogenicity with metformin was found in either male or female mice. Similarly, there was no tumorigenic potential observed with metformin in male rats. There was, however, an increased incidence of benign stromal uterine polyps in female rats treated with 900 mg/kg/day.
Mutagenesis
Ertugliflozin
Ertugliflozin was not mutagenic or clastogenic with or without metabolic activation in the microbial reverse mutation, in vitro cytogenetic (human lymphocytes), and in vivo rat micronucleus assays.
Metformin
There was no evidence of a mutagenic potential of metformin in the following in vitro tests: Ames test (S. typhimurium), gene mutation test (mouse lymphoma cells), or chromosomal aberrations test (human lymphocytes). Results in the in vivo mouse micronucleus test were also negative.
Impairment of Fertility
Ertugliflozin
In the rat fertility and embryonic development study, male and female rats were administered ertugliflozin at 5, 25, and 250 mg/kg/day. No effects on fertility were observed at 250 mg/kg/day (approximately 480 and 570 times male and female human exposures, respectively, at the MRHD of 15 mg/day based on AUC comparison).
Metformin HCl
Fertility of male or female rats was unaffected by metformin when administered at doses as high as 600 mg/kg/day, which is approximately three times the maximum recommended human daily dose based on body surface area comparisons.
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
14.1 Glycemic Control Trials in Patients with Type 2 Diabetes Mellitus
The efficacy and safety of ertugliflozin in combination with metformin have been studied in 4 multicenter, randomized, double-blind, placebo- and active comparator-controlled, clinical studies involving 3,643 patients with type 2 diabetes mellitus. These studies included White, Hispanic, Black, Asian, and other racial and ethnic groups, and patients with an age range of 21 to 86 years.
In VERTIS CV, ertugliflozin has been studied as add on to insulin (with or without metformin) and as add on to metformin plus a sulfonylurea in substudies.
In patients with type 2 diabetes mellitus, treatment with ertugliflozin in combination with metformin reduced hemoglobin A1c (HbA1c) compared to placebo.
In patients with type 2 diabetes mellitus treated with ertugliflozin in combination with metformin, the reduction in HbA1c was generally similar across subgroups defined by age, sex, race, geographic region, baseline body mass index (BMI), and duration of type 2 diabetes mellitus.
Ertugliflozin as Add-on Combination Therapy with Metformin
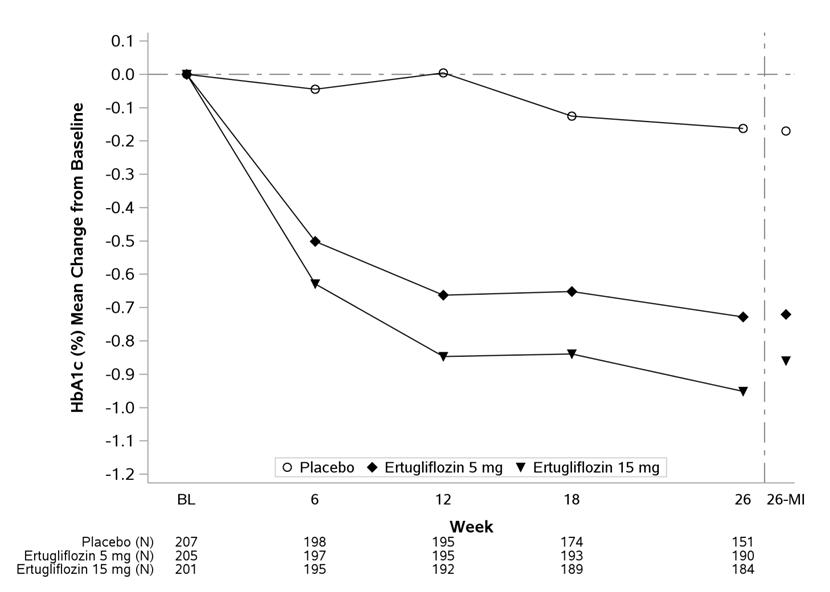
A total of 621 patients with type 2 diabetes mellitus inadequately controlled (HbA1c between 7% and 10.5%) on metformin monotherapy (≥1,500 mg/day for ≥8 weeks) participated in a randomized, double-blind, multi-center, 26-week, placebo-controlled study (NCT02033889) to evaluate the efficacy and safety of ertugliflozin in combination with metformin. Patients entered a 2-week, single-blind, placebo run-in, and were randomized to placebo, ertugliflozin 5 mg, or ertugliflozin 15 mg administered once daily in addition to continuation of background metformin therapy.
At Week 26, statistically significant reductions in HbA1c were observed in the ertugliflozin 5 mg and 15 mg groups compared to placebo. Ertugliflozin also resulted in a greater proportion of patients achieving an HbA1c <7% compared to placebo (see Table 6 and Figure 3).
Table 6: Results at Week 26 from a Placebo-Controlled Study for Ertugliflozin Used in Combination with Metformin in Patients with Type 2 Diabetes Mellitus*|
Placebo |
Ertugliflozin 5 mg |
Ertugliflozin 15 mg | |
|---|---|---|---|
| |||
|
HbA1c (%) |
N = 207 |
N = 205 |
N = 201 |
|
Baseline (mean) |
8.2 |
8.1 |
8.1 |
|
Change from baseline (LS mean†) |
-0.2 |
-0.7 |
-0.9 |
|
Difference from placebo (LS mean†, 95% CI) |
-0.5‡ (-0.7, -0.4) |
-0.7‡ (-0.9, -0.5) | |
|
Patients [N (%)] with HbA1c <7% |
38 (18.4) |
74 (36.3) |
87 (43.3) |
|
FPG (mg/dL) |
N = 202 |
N = 199 |
N = 201 |
|
Baseline (mean) |
169.1 |
168.1 |
167.9 |
|
Change from baseline (LS mean†) |
-8.7 |
-30.3 |
-40.9 |
|
Difference from placebo (LS mean†, 95% CI) |
-21.6‡ (-27.8, -15.5) |
-32.3‡ (-38.5, -26.0) |
The mean baseline body weight was 84.5 kg, 84.9 kg, and 85.3 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 26 were** -**1.4 kg, -3.2 kg, and -3.0 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The difference from placebo (95% CI) for ertugliflozin 5 mg was -1.8 kg (-2.4, -1.2) and for ertugliflozin 15 mg was -1.7 kg (-2.2, -1.1).
The mean baseline systolic blood pressure was 129.3 mmHg, 130.5 mmHg, and 130.2 mmHg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 26 were -1.8 mmHg, -5.1 mmHg, and -5.7 mmHg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The difference from placebo (95% CI) for ertugliflozin 5 mg was -3.3 mmHg (-5.6, -1.1) and for ertugliflozin 15 mg was -3.8 mmHg (-6.1, -1.5).
|
|
Figure 3: HbA1c (%) Change over Time in a 26-Week Placebo-Controlled Study for Ertugliflozin Used in Combination with Metformin in Patients with Type 2 Diabetes Mellitus***** |
|
|
In Combination with Sitagliptin versus Ertugliflozin Alone and Sitagliptin Alone, as Add-on to Metformin
A total of 1,233 patients with type 2 diabetes mellitus with inadequate glycemic control (HbA1c between 7.5% and 11%) on metformin monotherapy (≥1,500 mg/day for ≥8 weeks) participated in a randomized, double-blind, 26-week, active controlled study (NCT02099110) to evaluate the efficacy and safety of ertugliflozin 5 mg or 15 mg in combination with sitagliptin 100 mg compared to the individual components. Patients were randomized to one of five treatment arms: ertugliflozin 5 mg, ertugliflozin 15 mg, sitagliptin 100 mg, ertugliflozin 5 mg + sitagliptin 100 mg, or ertugliflozin 15 mg + sitagliptin 100 mg.
At Week 26, ertugliflozin 5 mg or 15 mg + sitagliptin 100 mg provided statistically significantly greater reductions in HbA1c compared to ertugliflozin (5 mg or 15 mg) alone or sitagliptin 100 mg alone. The mean change from baseline in HbA1c was -1.4% for ertugliflozin 5 mg or 15 mg + sitagliptin 100 mg versus -1.0%, for ertugliflozin 5 mg, ertugliflozin 15 mg, or sitagliptin 100 mg, respectively. More patients receiving ertugliflozin 5 mg or 15 mg + sitagliptin 100 mg achieved an HbA1c <7% (53.3% and 50.9%, for ertugliflozin 5 mg or 15 mg, respectively, + sitagliptin 100 mg) compared to the individual components (29.3%, 33.7%, and 38.5% for ertugliflozin 5 mg, ertugliflozin 15 mg, or sitagliptin 100 mg, respectively).
Ertugliflozin as Add-on Combination Therapy with Metformin and Sitagliptin
A total of 463 patients with type 2 diabetes mellitus inadequately controlled (HbA1c between 7% and 10.5%) on metformin (≥1,500 mg/day for ≥8 weeks) and sitagliptin 100 mg once daily participated in a randomized, double-blind, multi-center, 26-week, placebo-controlled study (NCT02036515) to evaluate the efficacy and safety of ertugliflozin. Patients entered a 2-week, single-blind, placebo run-in period and were randomized to placebo, ertugliflozin 5 mg, or ertugliflozin 15 mg.
At Week 26, treatment with ertugliflozin at 5 mg or 15 mg daily provided statistically significant reductions in HbA1c. Ertugliflozin also resulted in a higher proportion of patients achieving an HbA1c <7% compared to placebo (see Table 7).
Table 7: Results at Week 26 from an Add-on Study of Ertugliflozin in Combination with Metformin and Sitagliptin in Patients with Type 2 Diabetes Mellitus*|
Placebo |
Ertugliflozin 5 mg |
Ertugliflozin 15 mg | |
|---|---|---|---|
| |||
|
HbA1c (%) |
N = 152 |
N = 155 |
N = 152 |
|
Baseline (mean) |
8.0 |
8.1 |
8.0 |
|
Change from baseline (LS mean†) |
-0.2 |
-0.7 |
-0.8 |
|
Difference from placebo (LS mean†, 95% CI) |
-0.5‡ (-0.7, -0.3) |
-0.6‡ (-0.8, -0.4) | |
|
Patients [N (%)] with HbA1c <7% |
31 (20.2) |
54 (34.6) |
64 (42.3) |
|
FPG (mg/dL) |
N = 152 |
N = 156 |
N = 152 |
|
Baseline (mean) |
169.6 |
167.7 |
171.7 |
|
Change from baseline (LS mean†) |
-6.5 |
-25.7 |
-32.1 |
|
Difference from placebo (LS mean†, 95% CI) |
-19.2‡ (-26.8, -11.6) |
-25.6‡ (-33.2, -18.0) |
The mean baseline body weight was 86.5 kg, 87.6 kg, and 86.6 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 26 were -1.0 kg, -3.0 kg, and -2.8 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The difference from placebo (95% CI) for ertugliflozin 5 mg was -1.9 kg (-2.6, -1.3) and for ertugliflozin 15 mg was -1.8 kg (-2.4, -1.2).
The mean baseline systolic blood pressure was 130.2 mmHg, 132.1 mmHg, and 131.6 mmHg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 26 were -0.2 mmHg, -3.8 mmHg, and -4.5 mmHg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The difference from placebo (95% CI) for ertugliflozin 5 mg was -3.7 mmHg (-6.1, -1.2) and for ertugliflozin 15 mg was -4.3 mmHg (-6.7, -1.9).
Active Controlled Study of Ertugliflozin Versus Glimepiride as Add-on Combination Therapy with Metformin
A total of 1,326 patients with type 2 diabetes mellitus inadequately controlled (HbA1c between 7% and 9%) on metformin monotherapy participated in a randomized, double-blind, multi-center, 52-week, active comparator- controlled study (NCT01999218) to evaluate the efficacy and safety of ertugliflozin in combination with metformin. These patients, who were receiving metformin monotherapy (≥1,500 mg/day for ≥8 weeks), entered a 2-week, single-blind, placebo run-in period and were randomized to glimepiride, ertugliflozin 5 mg, or ertugliflozin 15 mg administered once daily in addition to continuation of background metformin therapy. Glimepiride was initiated at 1 mg/day and titrated up to a maximum dose of 6 or 8 mg/day (depending on maximum approved dose in each country) or a maximum tolerated dose or down-titrated to avoid or manage hypoglycemia. The mean daily dose of glimepiride was 3.0 mg.
Ertugliflozin 15 mg was non-inferior to glimepiride after 52 weeks of treatment. (See Table 8.)
Table 8: Results at Week 52 from an Active-Controlled Study Comparing Ertugliflozin to Glimepiride as Add-on Therapy in Patients with Type 2 Diabetes Mellitus Inadequately Controlled on Metformin*|
Glimepiride |
Ertugliflozin 5 mg |
Ertugliflozin 15 mg | |
|---|---|---|---|
| |||
|
HbA1c (%) |
N = 437 |
N = 447 |
N = 440 |
|
Baseline (mean) |
7.8 |
7.8 |
7.8 |
|
Change from baseline (LS mean†) |
-0.6 |
-0.5 |
-0.5 |
|
Difference from glimepiride (LS mean†, 95% CI) |
0.2‡ (0.0, 0.3) |
0.1‡ (-0.0, 0.2) | |
|
Patients [N (%)] with HbA1c <7% |
208 (47.7) |
177 (39.5) |
186 (42.2) |
The mean baseline body weight was 86.8 kg, 87.9 kg, and 85.6 kg in the glimepiride, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 52 were 0.6 kg, -2.6 kg, and -3.0 kg in the glimepiride, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The difference from glimepiride (95% CI) for ertugliflozin 5 mg was -3.2 kg (-3.7, -2.7) and for ertugliflozin 15 mg was -3.6 kg (-4.1, -3.1).
Ertugliflozin as Add-on Combination Therapy with Insulin (With or Without Metformin)
In an 18-week randomized, double-blind, multi-center, placebo-controlled, glycemic sub-study of VERTIS CV (NCT01986881, study details see 14.2), a total of 1065 patients with type 2 diabetes mellitus and established atherosclerotic cardiovascular disease with inadequate glycemic control (HbA1c between 7% and 10.5%) on background therapy of insulin ≥20 units/day (59% also on metformin ≥1,500 mg/day) were randomized to placebo, ertugliflozin 5 mg or ertugliflozin 15 mg once daily treatment.
At Week 18, treatment with ertugliflozin at 5 mg or 15 mg daily provided statistically significant reductions in HbA1c compared to placebo (see Table 9).
Table 9: Results at Week 18 from an Add-on Study of Ertugliflozin in Combination with Insulin (with or without Metformin) in Patients with Type 2 Diabetes Mellitus*|
Placebo |
Ertugliflozin 5 mg |
Ertugliflozin 15 mg | |
|---|---|---|---|
|
SE: standard error. | |||
| |||
|
HbA1c (%) |
N = 346 |
N = 346 |
N = 367 |
|
Baseline (mean) |
8.4 |
8.4 |
8.4 |
|
Change from baseline (LS mean†, SE) |
-0.2 (0.05) |
-0.7 (0.05) |
-0.7 (0.05) |
|
Difference from placebo (LS mean†, 95% CI) |
-0.5‡ (-0.6, -0.4) |
-0.5‡ (-0.7, -0.4) | |
|
Patients [N (%)] with HbA1c <7%§ |
37 (10.7) |
79 (22.8) |
81 (22.1) |
|
FPG (mg/dL) |
N = 343 |
N = 346 |
N = 368 |
|
Baseline (mean) |
167.4 |
173.8 |
175.4 |
|
Change from baseline (LS mean†, SE) |
-6.3 (2.91) |
-25.6 (2.90) |
-29.8 (2.86) |
|
Difference from placebo (LS mean†, 95% CI) |
-19.2‡ (-26.8, -11.6) |
-23.4‡ (-30.9, -16.0) |
The mean baseline body weights were 93.3 kg, 93.8 kg, and 92.1 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 18 were -0.2 kg, - 1.6 kg, and -1.9 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The differences from placebo (95% CI) for ertugliflozin 5 mg were - 1.4 kg (- 1.9, - 0.9) and for ertugliflozin 15 mg was -1.6 kg (-2.1, -1.1).
The mean baseline systolic blood pressures were 134.0 mmHg, 135.6 mmHg, and 133.7 mmHg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 18 were 0.7 mmHg, -2.2 mmHg, and -1.7 mmHg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The differences from placebo (95% CI) for ertugliflozin 5 mg was – 2.9 mmHg (-4.9, -1.0) and for ertugliflozin 15 mg were -2.5 mmHg (- 4.4, - 0.5).
Add-on Combination Therapy with Metformin and Sulfonylurea
In an 18-week randomized, double-blind, multi-center, placebo-controlled, glycemic sub-study of VERTIS CV (NCT01986881, study details see 14.2), a total of 330 patients with type 2 diabetes mellitus and established atherosclerotic cardiovascular disease with inadequate glycemic control (HbA1c between 7% and 10.5%) with background therapy of metformin ≥1,500 mg/day and a sulfonylurea (SU) were randomized to placebo, ertugliflozin 5 mg or ertugliflozin 15 mg once daily treatment.
At Week 18, treatment with ertugliflozin at 5 mg or 15 mg daily provided statistically significant reductions in HbA1c compared to placebo (see Table 10).
Table 10: Results at Week 18 from an Add-on Study of Ertugliflozin in Combination with Metformin and a SU in Patients with Type 2 Diabetes Mellitus*|
Placebo |
Ertugliflozin 5 mg |
Ertugliflozin 15 mg | |
|---|---|---|---|
|
SE: standard error | |||
| |||
|
HbA1c (%) |
N = 116 |
N = 99 |
N = 113 |
|
Baseline (mean) |
8.3 |
8.4 |
8.3 |
|
Change from baseline (LS mean†, SE) |
-0.3 (0.08) |
-0.8 (0.09) |
-0.9 (0.08) |
|
Difference from placebo (LS mean†, 95% CI) |
-0.6‡ (-0.8, -0.3) |
-0.7‡ (-0.9, -0.4) | |
|
Patients [N (%)] with HbA1c <7%****§ |
17 (14.7) |
39 (39.4) |
38 (33.6) |
|
FPG (mg/dL) |
N = 117 |
N = 99 |
N = 113 |
|
Baseline (mean) |
177.3 |
183.5 |
174.0 |
|
Change from baseline (LS mean†, SE) |
-3.5 (3.65) |
-31.3 (3.87) |
-33.0 (3.67) |
|
Difference from placebo (LS mean†, 95% CI) |
-27.9‡ (-37.8, -17.9) |
-29.5‡ (-39.0, -19.9) |
The mean baseline body weights were 90.5 kg, 92.1 kg, and 92.9 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The mean changes from baseline to Week 18 were - 0.6 kg, -2.0 kg, and - 2.2 kg in the placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg groups, respectively. The differences from placebo (95% CI) for ertugliflozin 5 mg were - 1.4 kg (- 2.2, - 0.7) and for ertugliflozin 15 mg was - 1.6 kg (- 2.3, - 0.9).
14.2 Ertugliflozin Cardiovascular Outcomes in Patients with Type 2 Diabetes
and Established Cardiovascular Disease
The effect of ertugliflozin on cardiovascular risk in adult patients with type 2 diabetes and established atherosclerotic cardiovascular disease was evaluated in the VERTIS CV study (NCT 01986881), a multicenter, multi- national, randomized, double-blind, placebo-controlled, event-driven trial. The study compared the risk of experiencing a major adverse cardiovascular event (MACE) between ertugliflozin and placebo when these were added to and used concomitantly with standard of care treatments for diabetes and atherosclerotic cardiovascular disease.
A total of 8246 patients were randomized (placebo N=2747, ertugliflozin 5 mg N=2752, ertugliflozin 15 mg N=2747) and followed for a median of 3 years. Approximately 88% of the study population was Caucasian, 6% Asian, and 3% Black. The mean age was 64 years and approximately 70% were male.
All patients in the study had inadequately controlled type 2 diabetes mellitus at baseline (HbA1c greater than or equal to 7%). The mean duration of type 2 diabetes mellitus was 13 years, the mean HbA1c at baseline was 8.2% and the mean eGFR was 76 mL/min/1.73 m2. At baseline, patients were treated with one (32%) or more (67%) antidiabetic medications including biguanides (metformin) (76%), insulin (47%), sulfonylureas (41%), DPP-4 inhibitors (11%) and GLP-1 receptor agonists (3%).
Almost all patients (99%) had established atherosclerotic cardiovascular disease at baseline including: a documented history of coronary artery disease (76%), cerebrovascular disease (23%) or peripheral artery disease (19%). Approximately 24% patients had a history of heart failure (HF). At baseline, the mean systolic blood pressure was 133 mmHg, the mean diastolic blood pressure was 77 mmHg, the mean LDL was 89 mg/dL, and the mean HDL was 44 mg/dL. At baseline, approximately 81% of patients were treated with renin angiotensin system inhibitors, 69% with beta-blockers, 43% with diuretics, 82% with statins, 4% ezetimibe, and 89% with antiplatelet agents.
The primary endpoint in VERTIS CV was the time to first occurrence of a Major Adverse Cardiac Event (MACE). A major adverse cardiovascular event was defined as occurrence of either a cardiovascular death or a nonfatal myocardial infarction (MI) or a nonfatal stroke. The statistical analysis plan pre- specified that the 5 and 15 mg doses would be combined for the analysis. A Cox proportional hazards model was used to test for non-inferiority against the pre-specified risk margin of 1.3 for the hazard ratio of MACE. Type-1 error was controlled across multiple tests using a hierarchical testing strategy.
The incidence rate of MACE was similar between the ertugliflozin-treated and placebo-treated patients. The estimated hazard ratio of MACE associated with ertugliflozin relative to placebo was 0.97 with 95.6% confidence interval (0.85, 1.11). The upper bound of this confidence interval excluded a risk larger than 1.3 (Table 11). Results for the 5 mg and 15 mg doses were consistent with results for the combined dose group.
Table 11: Analysis of MACE and its Components from the VERTIS-CV Study*|
Endpoint† |
Placebo (N=2747) |
ertugliflozin (N=5499) |
Hazard Ratio vs Placebo | ||
|---|---|---|---|---|---|
|
N (%) |
Event Rate (per 100 person-years) |
N (%) |
Event Rate (per 100 person-years) | ||
|
N=Number of patients, CI=Confidence interval, CV=Cardiovascular, MI=Myocardial infarction. | |||||
| |||||
|
MACE (CV death, non-fatal MI, or non-fatal stroke) Composite |
327 (11.9) |
4.0 |
653 (11.9) |
3.9 |
0.97 |
|
Components of Composite Endpoint | |||||
|
Non-fatal MI |
148 (5.4) |
1.6 |
310 (5.6) |
1.7 |
1.04 |
|
Non-fatal Stroke |
78 (2.8) |
0.8 |
157 (2.9) |
0.8 |
1.00 |
|
CV death |
184 (6.7) |
1.9 |
341 (6.2) |
1.8 |
0.92 |
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
Product: 50090-6218
NDC: 50090-6218-0 60 TABLET, FILM COATED in a BOTTLE
INFORMATION FOR PATIENTS SECTION
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Lactic Acidosis
Inform patients of the risks of lactic acidosis due to the metformin component, its symptoms, and conditions that predispose to its development [see Warnings and Precautions (5.1)]. Advise patients to discontinue SEGLUROMET immediately and to notify their doctor promptly if unexplained hyperventilation, malaise, myalgia, unusual somnolence, slow or irregular heartbeat, sensation of feeling cold (especially in the extremities), or other nonspecific symptoms occur. GI symptoms are common during initiation of metformin treatment and may occur during initiation of SEGLUROMET therapy; however, advise patients to consult their doctor if they develop unexplained symptoms. Although GI symptoms that occur after stabilization are unlikely to be drug related, such an occurrence of symptoms should be evaluated to determine if it may be due to metformin-induced lactic acidosis or other serious disease.
Ketoacidosis
Inform patients that ketoacidosis is a serious life-threatening condition and that cases of ketoacidosis have been reported during use of medicines containing SGLT2 inhibitors, including ertugliflozin, sometimes associated with illness or surgery among other risk factors. Instruct patients to check ketones (when possible) if symptoms consistent with ketoacidosis occur even if blood glucose is not elevated. If symptoms of ketoacidosis (including nausea, vomiting, abdominal pain, tiredness, and labored breathing) occur, instruct patients to discontinue SEGLUROMET and seek medical attention immediately [see Warnings and Precautions (5.2)].
Amputation
Inform patients of the potential for an increased risk of amputations. Counsel patients about the importance of routine preventative foot care. Instruct patients to monitor for new pain or tenderness, sores or ulcers, or infections involving the leg or foot and to seek medical advice immediately if such signs or symptoms develop [see Warnings and Precautions (5.3)].
Volume Depletion
Inform patients that symptomatic hypotension may occur with SEGLUROMET and advise them to contact their doctor if they experience such symptoms [see Warnings and Precautions (5.4)]. Inform patients that dehydration may increase the risk for hypotension, and to have adequate fluid intake.
Serious Urinary Tract Infections
Inform patients of the potential for urinary tract infections, which may be serious. Provide them with information on the symptoms of urinary tract infections. Advise them to seek medical advice if such symptoms occur [see Warnings and Precautions (5.5)].
Hypoglycemia with Concomitant Use of Insulin and/or Insulin Secretagogue
Inform patients that the incidence of hypoglycemia may increase when SEGLUROMET is added to insulin and/or an insulin secretagogue and that a lower dose of insulin or insulin secretagogue may be required to reduce the risk of hypoglycemia [see Warnings and Precautions (5.6)].
Necrotizing Fasciitis of the Perineum (Fournier's Gangrene)
Inform patients that necrotizing infections of the perineum (Fournier's Gangrene) have occurred with SGLT2 inhibitors. Counsel patients to promptly seek medical attention if they develop pain or tenderness, redness, or swelling of the genitals or the area from the genitals back to the rectum, along with a fever above 100.4°F or malaise [see Warnings and Precautions (5.7)].
Genital Mycotic Infections in Females (e.g., Vulvovaginitis)
Inform female patients that vaginal yeast infections may occur and provide them with information on the signs and symptoms of vaginal yeast infection. Advise them of treatment options and when to seek medical advice [see Warnings and Precautions (5.8)].
Genital Mycotic Infections in Males (e.g., Balanitis or Balanoposthitis)
Inform male patients that yeast infections of the penis (e.g., balanitis or balanoposthitis) may occur, especially in uncircumcised males. Provide them with information on the signs and symptoms of balanitis and balanoposthitis (rash or redness of the glans or foreskin of the penis). Advise them of treatment options and when to seek medical advice [see Warnings and Precautions (5.8)].
Fetal Toxicity
Advise pregnant patients of the potential risk to a fetus with treatment with SEGLUROMET. Instruct patients to immediately inform their healthcare provider if pregnant or planning to become pregnant [see Use in Specific Populations (8.1)].
Lactation
Advise patients that use of SEGLUROMET is not recommended while breastfeeding [see Use in Specific Populations (8.2)].
Pregnancy
Inform female patients that treatment with metformin may result in an unintended pregnancy in some premenopausal anovulatory females due to its effect on ovulation [see Use in Specific Populations (8.3)].
Laboratory Tests
Due to the mechanism of action of ertugliflozin, inform patients that their urine will test positive for glucose while taking SEGLUROMET.
Missed Dose
Instruct patients to take SEGLUROMET only as prescribed. If a dose is missed, it should be taken as soon as the patient remembers. Advise patients not to double their next dose.
SPL UNCLASSIFIED SECTION
Manufactured for: Merck Sharp & Dohme LLC
Rahway, NJ 07065, USA
For patent information: www.msd.com/research/patent
Copyright © 2017-2022 Merck & Co., Inc., Rahway, NJ, USA, and its affiliates.
All rights reserved.
uspi-mk8835b-t-2210r007
SPL MEDGUIDE SECTION
|
Medication Guide | |||
|---|---|---|---|
|
This Medication Guide has been approved by the U.S. Food and Drug Administration. |
Revised: 10/2022 | ||
|
Read this Medication Guide carefully before you start taking SEGLUROMET and each time you get a refill. There may be new information. This information does not take the place of talking with your doctor about your medical condition or your treatment. | |||
|
What is the most important information I should know about SEGLUROMET? | |||
|
| ||
|
Most people who have had lactic acidosis had other conditions that, in combination with metformin use, led to the lactic acidosis. Tell your doctor if you have any of the following, because you have a higher chance for getting lactic acidosis with SEGLUROMET if you:
The best way to keep from having a problem with lactic acidosis from metformin
is to tell your doctor if you have any of the problems in the list above. Your
doctor may decide to stop your SEGLUROMET for a while if you have any of these
things. | |||
|
What is SEGLUROMET?
| |||
|
Do not take SEGLUROMET if you:
| |||
|
Before you take SEGLUROMET, tell your doctor about all of your medical conditions, including if you:
**Tell your doctor about all of the medicines you take,**including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine. | |||
|
How should I take SEGLUROMET?
| |||
|
What should I avoid while taking SEGLUROMET?
| |||
|
What are the possible side effects of SEGLUROMET? ketoacidosis (increased ketones in your blood or urine).Ketoacidosis has happened in people who have type 1 diabetes or type 2 diabetesduring treatment with SEGLUROMET. Ketoacidosis has also happened in people with diabetes who were sick or who had surgery during treatment with SEGLUROMET. Ketoacidosis is a serious condition, which may need to be treated in a hospital. Ketoacidosis may lead to death.* Ketoacidosis can happen even if your blood sugar is less than 250 mg/dL. Stop taking SEGLUROMET and call your doctor right away if you get any of the following symptoms:** | |||
|
| ||
|
If you get any of these symptoms during treatment with SEGLUROMET, if possible, check for ketones in your urine, even if your blood sugar is less than 250 mg/dL. *Amputations. SEGLUROMET may increase your risk of lower limb amputations. Call your doctor right away if you have new pain or tenderness, any sores, ulcers, or infections in your leg or foot. Your doctor may decide to stop your SEGLUROMET for a while if you have any of these signs or symptoms. Talk to your doctor about proper foot care. *Dehydration. SEGLUROMET can cause some people to become dehydrated (the loss of body water and salt). Dehydration may cause you to feel dizzy, faint, lightheaded, or weak, especially when you stand up (orthostatic hypotension). There have been reports of sudden worsening of kidney function in people who are taking SEGLUROMET. Talk to your doctor about what you can do to prevent dehydration including how much fluid you should drink on a daily basis. ***serious urinary tract infections.**Serious urinary tract infections that may lead to hospitalization have happened in people who are taking SEGLUROMET. Tell your doctor if you have any signs or symptoms of a urinary tract infection such as a burning feeling when passing urine, a need to urinate often, the need to urinate right away, pain in the lower part of your stomach (pelvis), or blood in the urine. Sometimes people may also have a fever, back pain, nausea, or vomiting. ***low blood sugar (hypoglycemia).**If you take SEGLUROMET with another medicine that can cause low blood sugar such as a sulfonylurea or insulin, your risk of getting low blood sugar is higher. The dose of your sulfonylurea or insulin may need to be lowered while you take SEGLUROMET. Signs and symptoms of low blood sugar may include: | |||
|
|
| |
|
*a rare but serious bacterial infection that causes damage to the tissue under the skin (necrotizing fasciitis) in the area between and around the anus and genitals (perineum). Necrotizing fasciitis of the perineum has happened in women and men who take medicines that lower blood sugar in the same way as one of the medicines in SEGLUROMET. Necrotizing fasciitis of the perineum may lead to hospitalization, may require multiple surgeries, and may lead to death.Seek medical attention immediately if you have fever above 100.4°F or you are feeling very weak, tired or uncomfortable (malaise) and you develop any of the following symptoms in the area between and around your anus and genitals: | |||
|
|
| |
|
***vaginal yeast infection.**Women who take SEGLUROMET may get vaginal yeast infections. Symptoms of a vaginal yeast infection include: * vaginal odor * white or yellowish vaginal discharge (discharge may be lumpy or look like cottage cheese) * vaginal itching *yeast infection of the penis (balanitis or balanoposthitis). Men who take SEGLUROMET may get a yeast infection of the skin around the penis. Certain men who are not circumcised may have swelling of the penis that makes it difficult to pull back the skin around the tip of your penis. Other symptoms of yeast infection of the penis include: | |||
|
| ||
|
**Talk to your doctor about what to do if you get symptoms of a yeast infection of the vagina or penis.**Your doctor may suggest you use an over- the-counter antifungal medicine. Talk to your doctor right away if you use an over-the-counter antifungal medicine and your symptoms do not go away. low vitamin B**12***(vitamin B12deficiency).**Using metformin for long periods of time may cause a decrease in the amount of vitamin B12 in your blood, especially if you have had low vitamin B12 blood levels before. Your doctor may do blood tests to check your vitamin B12 levels. The most common side effects of ertugliflozin include:
The most common side effects of metformin hydrochloride include: | |||
|
|
| |
|
These are not all the possible side effects of SEGLUROMET. | |||
|
How should I store SEGLUROMET?
Keep SEGLUROMET and all medicines out of the reach of children. | |||
|
General information about the safe and effective use of SEGLUROMET. | |||
|
What are the ingredients in SEGLUROMET? | |||
|
Manufactured for: Merck Sharp & Dohme LLC |