
Manufacturing Establishments (1)
Quality Care Products, LLC
831276758
Products (1)
Methadone Hydrochloride
55700-882
ANDA090635
ANDA (C73584)
ORAL
October 26, 2020
Drug Labeling Information
DESCRIPTION SECTION
11 DESCRIPTION
Methadone hydrochloride is chemically described as 6-(dimethyl amino)-4,4-diphenyl-3-hepatanone hydrochloride. Methadone hydrochloride is a white, crystalline material that is water-soluble. Its molecular formula is C21H27NO•HCl and it has a molecular weight of 345.91. Methadone hydrochloride has a melting point of 235°C, and a pKa of 8.25 in water at 20°C. Its octanol/water partition coefficient at pH 7.4 is 117. A solution (1:100) in water has a pH between 4.5 and 6.5.
It has the following structural formula:
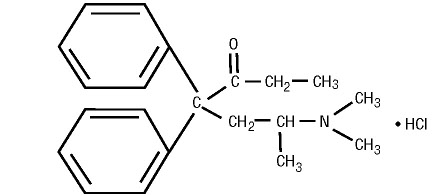
Each methadone hydrochloride tablets contains 10 mg of methadone hydrochloride, USP and the following inactive ingredients: magnesium stearate, microcrystalline cellulose, and starch.
CLINICAL PHARMACOLOGY SECTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Methadone hydrochloride is a mu-agonist; a synthetic opioid analgesic with multiple actions qualitatively similar to those of morphine, the most prominent of which involves the central nervous system and organs composed of smooth muscle. The principal therapeutic uses for methadone are for analgesia and for detoxification or maintenance in opioid addiction. The methadone withdrawal syndrome, although qualitatively similar to that of morphine, differs in that the onset is slower, the course is more prolonged, and the symptoms are less severe.
Some data also indicate that methadone acts as an antagonist at the N-methyl- D-aspartate (NMDA) receptor. The contribution of NMDA receptor antagonism to methadone’s efficacy is unknown.
12.3 Pharmacokinetics
Absorption:
Following oral administration the bioavailability of methadone ranges between
36 to 100% and peak plasma concentrations are achieved between 1 to 7.5 hours.
Dose proportionality of methadone pharmacokinetics is not known. However,
after administration of daily oral doses ranging from 10 to 225 mg, the
steady-state plasma concentrations ranged between 65 to 630 ng/mL and the peak
concentrations ranged between 124 to 1255 ng/mL. Effect of food on the
bioavailability of methadone has not been evaluated.
Distribution:
Methadone is a lipophilic drug and the steady-state volume of distribution
ranges between 1.0 to 8.0 L/kg. In plasma, methadone is predominantly bound to
α-acid glycoprotein (85% to 90%). Methadone is secreted in saliva, breast
milk, amniotic fluid and umbilical cord plasma.
Elimination
Metabolism: Methadone is primarily metabolized by N-demethylation to an
inactive metabolite, 2-ethylidene-1, 5-dimethyl-3, 3-diphenylpyrrolidene
(EDDP). Cytochrome P450 enzymes, primarily CYP3A4, CYP2B6, CYP2C19, CYP2C9 and
CYP2D6, are responsible for conversion of methadone to EDDP and other inactive
metabolites, which are excreted mainly in the urine. Methadone appears to be a
substrate for P-glycoprotein but its pharmacokinetics do not appear to be
significantly altered in case of P-glycoprotein polymorphism or inhibition.
Excretion: The elimination of methadone is mediated by extensive biotransformation, followed by renal and fecal excretion. Published reports indicate that after multiple dose administration the apparent plasma clearance of methadone ranged between 1.4 and 126 L/h, and the terminal half-life (T1/2) was highly variable and ranged between 8 to 59 hours in different studies. Methadone is a basic (pKa=9.2) compound and the pH of the urinary tract can alter its disposition in plasma. Also, since methadone is lipophilic, it has been known to persist in the liver and other tissues. The slow release from the liver and other tissues may prolong the duration of methadone action despite low plasma concentrations.
Drug Interaction Studies
Cytochrome P450 Interactions: Methadone undergoes hepatic N-demethylation by
cytochrome P450 (CYP) isoforms, principally CYP3A4, CYP2B6, CYP2C19, CYP2C9
and CYP2D6. Co-administration of methadone with CYP inducers may result in
more rapid metabolism and potential for decreased effects of methadone,
whereas administration with CYP inhibitors may reduce metabolism and
potentiate methadone’s effects. Although antiretroviral drugs such as
efavirenz, nelfinavir, nevirapine, ritonavir, lopinavir+ritonavir combination
are known to inhibit some CYPs, they are shown to reduce the plasma levels of
methadone, possibly due to CYP induction activity [see Drug Interactions (7)].
Cytochrome P450 Inducers: The following drug interactions were reported following co-administration of methadone with known inducers of cytochrome P450 enzymes:
Rifampin: In patients well-stabilized on methadone, concomitant administration of rifampin resulted in a marked reduction in serum methadone levels and a concurrent appearance of withdrawal symptoms.
Phenytoin:In a pharmacokinetic study with patients on methadone maintenance therapy, phenytoin administration (250 mg twice daily initially for 1 day followed by 300 mg daily for 3 to 4 days) resulted in an approximately 50% reduction in methadone exposure and withdrawal symptoms occurred concurrently. Upon discontinuation of phenytoin, the incidence of withdrawal symptoms decreased and methadone exposure increased to a level comparable to that prior to phenytoin administration.
St. John’s Wort, Phenobarbital, Carbamazepine: Administration of methadone with other CYP3A4 inducers may result in withdrawal symptoms.
Cytochrome P450 Inhibitors:
Voriconazole: Voriconazole can inhibit the activity of CYP3A4, CYP2C9, and
CYP2C 19. Repeat dose administration of oral Voriconazole (400 mg every 12
hours for 1 day, then 200 mg every 12 hours for 4 days) increased the peak
plasma concentration (Cmax) and AUC of (R)-methadone by 31% and 47%,
respectively, in subjects receiving a methadone maintenance dose (30 to 100 mg
daily. The Cmax and AUC of (S)-methadone increased by 65% and 103%,
respectively. Increased plasma concentrations of methadone have been
associated with toxicity including QT prolongation. Frequent monitoring for
adverse events and toxicity related to methadone is recommended during co-
administration. Dose reduction of methadone may be needed [see Drug Interactions (7)].
Antiretroviral Drugs: Although antiretroviral drugs such as efavirenz,
nelfinavir, nevirapine, ritonavir, telaprevir, lopinavir+ritonavir combination
are known to inhibit some CYPs, they are shown to reduce the plasma levels of
methadone, possibly due to CYP induction activity.
Abacavir, Amprenavir, Darunavir+Ritonavir, Efavirenz, Nelfinavir, Nevirapine,
Ritonavir, Telaprevir, Lopinavir+Ritonavir, Saquinavir+Ritonavir,
Tipranavir+Ritonavir Combination: Co-administration of these anti-retroviral
agents resulted in increased clearance or decreased plasma levels of methadone
[see Drug Interactions (7)].
Didanosine and Stavudine: Methadone decreased the AUC and peak levels for didanosine and stavudine, with a more significant decrease for didanosine. Methadone disposition was not substantially altered [see Drug Interactions (7)].
Zidovudine:Methadone increased the AUC of zidovudine which could result in toxic effects [see Drug Interactions (7)].
INDICATIONS & USAGE SECTION
Highlight: Methadone hydrochloride tablets, USP is an opioid agonist indicated for the:
- Management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.
Limitations of Use
* Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, and because of the greater risks of overdose and death with long-acting opioids, reserve Methadone Hydrochloride for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain.
* Methadone hydrochloride tablets are not indicated as an as-needed (prn) analgesic.
2. Detoxification treatment of opioid addiction (heroin or other morphine-like drugs). 3. Maintenance treatment of opioid addiction (heroin or other morphine-like drugs), in conjunction with appropriate social and medical services. (1)
1 INDICATIONS AND USAGE
Methadone hydrochloride tablets, USP are indicated for the:
- Management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.
Limitations of Use
* Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, and because of the greater risks of overdose and death with long-acting opioids [see Warnings and Precautions (5.1)], reserve methadone hydrochloride tablets for use in patients for whom alternative analgesic treatment options (e.g., non-opioid analgesics or immediate-release opioid analgesics) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain.
* Methadone hydrochloride tablets are not indicated as an as-needed (prn) analgesic.
2. Detoxification treatment of opioid addiction (heroin or other morphine-like drugs). 3. Maintenance treatment of opioid addiction (heroin or other morphine-like drugs), in conjunction with appropriate social and medical services.
Conditions for Distribution and Use of Methadone Products for the Treatment of Opioid Addiction
Code of Federal Regulations, Title 42, Sec 8: Methadone products when used
for the treatment of opioid addiction in detoxification or maintenance
programs, shall be dispensed only by opioid treatment programs (and agencies,
practitioners or institutions by formal agreement with the program sponsor)
certified by the Substance Abuse and Mental Health Services Administration and
approved by the designated state authority. Certified treatment programs shall
dispense and use methadone in oral form only and according to the treatment
requirements stipulated in the Federal Opioid Treatment Standards (42 CFR
8.12). See below for important regulatory exceptions to the general
requirement for certification to provide opioid agonist treatment.
Failure to abide by the requirements in these regulations may result in
criminal prosecution, seizure of the drug supply, revocation of the program
approval, and injunction precluding operation of the program.
Regulatory Exceptions to the General Requirement for Certification to Provide Opioid Agonist Treatment:
- During inpatient care, when the patient was admitted for any condition other than concurrent opioid addiction (pursuant to 21CFR 1306.07(c)), to facilitate the treatment of the primary admitting diagnosis).
- During an emergency period of no longer than 3 days while definitive care for the addiction is being sought in an appropriately licensed facility (pursuant to 21CFR 1306.07(b)).
DOSAGE & ADMINISTRATION SECTION
Highlight: Management of Pain
- To be prescribed only by healthcare providers knowledgeable in use of potent opioids for management of chronic pain. (2.3)
- Use the lowest effective dosage for the shortest duration consistent with individual patient treatment goals. (2.3)
- Individualize dosing based on the severity of pain, patient response, prior analgesic experience, and risk factors for addiction, abuse, and misuse (2.3)
- For opioid naïve patients, initiate methadone hydrochloride tablets treatment with 2.5 mg every 8 to 12 hours. (2.3)
- To convert to methadone hydrochloride tablets from another opioid, use available conversion factors to obtain estimated dose. (2.3)
- Titrate slowly with dose increases no more frequent than every 3 to 5 days. (2.4)
- Do not abruptly discontinue methadone hydrochloride tablets in a physically dependent patient. (2.5, 5.15)
Initiation of Detoxification and Maintenance Treatment
- A single dose of 20 to 30 mg may be sufficient to suppress withdrawal syndrome. (2.6)
2 DOSAGE AND ADMINISTRATION
2.1 Important General Information
- The peak respiratory depressant effect of methadone occurs later and persists longer than its peak therapeutic effect.
- A high degree of opioid tolerance does not eliminate the possibility of methadone overdose, iatrogenic or otherwise. Deaths have been reported during conversion to methadone from chronic, high-dose treatment with other opioid agonists and during initiation of methadone treatment of addiction in subjects previously abusing high doses of other agonists.
- Methadone has a narrow therapeutic index, especially when combined with other drugs.
2.2 Initial Dosing for Management of Pain
Important Dosage and Administration Information
Methadone Hydrochloride tablets should be prescribed only by healthcare
professionals who are knowledgeable in the use of potent opioids for the
management of chronic pain.
Consider the following important factors that differentiate methadone from other opioid analgesics:
- There is high interpatient variability in absorption, metabolism, and relative analgesic potency of methadone. Population-based equianalgesic conversion ratios between methadone and other opioids are not accurate when applied to individuals.
- The duration of analgesic action of methadone is 4 to 8 hours (based on single-dose studies) but the plasma elimination half-life is 8 to 59 hours.
- With repeated dosing, the potency of methadone increases due to systemic accumulation.
- Steady-state plasma concentrations and full analgesic effects are not attained until at least 3 to 5 days on a dose, and may take longer in some patients.
Use the lowest effective dosage for the shortest duration consistent with individual patient treatment goals [see Warnings and Precautions (5)].
Initiate the dosing regimen for each patient individually, taking into account the patient’s severity of pain, patient response, prior analgesic treatment experience, and risk factors for addiction, abuse, and misuse [see Warnings and Precautions (5.1)]. Monitor patients closely for respiratory depression, especially within the first 24 to 72 hours of initiating therapy with methadone hydrochloride tablets and adjust the dosage accordingly [see Warnings and Precautions (5.3)].
Use of Methadone hydrochloride tablets, USP as the First Opioid Analgesic
Initiate treatment with Methadone hydrochloride tablets with 2.5 mg orally
every 8 to 12 hours.
Conversion from Other Oral Opioids to methadone hydrochloride tablets, USP
Discontinue all other around-the-clock opioid drugs when methadone
hydrochloride tablets therapy is initiated. Deaths have occurred in opioid-
tolerant patients during conversion to methadone.
The potency of methadone relative to other opioid analgesics is nonlinear and increases with increasing dose. Table 1 provides an estimated conversion factor for use when converting patients from another opioid to methadone. Because of the high inter-patient variability in absorption, metabolism, and relative potency, it is critical to avoid overestimating the methadone dose which can lead to fatal respiratory depression. It is safer to underestimate a patient’s 24-hour methadone dosage and provide rescue medication (e.g., immediate-release opioid) than to overestimate the 24-hour methadone dosage and manage an adverse reaction due to an overdose.
Consider the following when using the information in Table 1:
- This is not a table of equianalgesic doses.
- The conversion factors in this table are only for the conversionfrom another oral opioid analgesicto methadone hydrochloride tablets.
- The tablecannot be used to convert from methadone hydrochloride tablets to another opioid. Doing so will result in an overestimation of the dose of the new opioid and may result in fatal overdose.
|
Total Daily Baseline Oral Morphine Equivalent Dose |
Estimated Daily Oral Methadone Requirement as Percent of Total Daily Morphine Equivalent Dose |
|
< 100 mg |
20% to 30% |
|
100 to 300 mg |
10% to 20% |
|
300 to 600 mg |
8% to 12% |
|
600 mg to 1,000 mg |
5% to 10% |
|
< 5 % |
To calculate the estimated methadone hydrochloride tablets dose using Table 1:
- For patients on a single opioid, sum the current total daily dose of the opioid, convert it to a Morphine Equivalent Dose according to specific conversion factor for that specific opioid, then multiply the Morphine Equivalent Dose by the corresponding percentage in the above table to calculate the approximate oral methadone daily dose. Divide the total daily methadone dose derived from the table above to reflect the intended dosing schedule (i.e., for administration every 8 hours, divide total daily methadone dose by 3).
- For patients on a regimen of more than one opioid, calculate the approximate oral methadone dose for each opioid and sum the totals to obtain the approximate total methadone daily dose. Divide the total daily methadone dose derived from the table above to reflect the intended dosing schedule (i.e., for administration every 8 hours, divide total daily methadone dose by 3).
- For patients on a regimen of fixed-ratio opioid/non-opioid analgesic products, use only the opioid component of these products in the conversion.
Always round the dose down, if necessary, to the appropriate methadone
hydrochloride tablets strength(s) available.
Example conversion from a single opioid to methadone hydrochloride tablets:
Step 1:
Sum the total daily dose of the opioid (in this case, Morphine Extended
Release Tablets 50 mg twice daily)
50 mg Morphine Extended Release Tablets 2 times daily = 100 mg total daily
dose of Morphine
Step 2:
Calculate the approximate equivalent dose of Methadone Hydrochloride Tablets
based on the total daily dose of Morphine using Table 1.
100 mg total daily dose of Morphine x 15% (10% to 20% per Table 1) = 15 mg
methadone hydrochloride tablets daily
Step 3:
Calculate the approximate starting dose of methadone hydrochloride tablets to
be given every 12 hours. Round down, if necessary, to the appropriate
methadone hydrochloride tablets strengths available.
15 mg daily / 2 = 7.5 mg methadone hydrochloride tablets every 12 hours
Then 7.5 mg is rounded down to 5 mg methadone hydrochloride tablets every 12
hours
Close observation and frequent titration are warranted until pain management is stable on the new opioid. Monitor patients for signs and symptoms of opioid withdrawal or for signs of over-sedation/toxicity after converting patients to methadone hydrochloride tablets.
Conversion from Parenteral Methadone to methadone hydrochloride tablets
Use a conversion ratio of 1:2 mg for parenteral to oral methadone (e.g., 5 mg
parenteral methadone to 10 mg oral methadone).
2.3 Titration and Maintenance of Therapy for Pain
Individually titrate methadone hydrochloride tablets to a dose that provides adequate analgesia and minimizes adverse reactions. Continually reevaluate patients receiving methadone hydrochloride tablets to assess the maintenance of pain control and the relative incidence of adverse reactions, as well as monitoring for the development of addiction, abuse, or misuse. Frequent communication is important among the prescriber, other members of the healthcare team, the patient, and the caregiver/family during periods of changing analgesic requirements, including initial titration. During chronic therapy, periodically reassess the continued need for the use of opioid analgesics.
Patients who experience breakthrough pain may require a dose increase of
methadone hydrochloride tablets, or may need rescue medication with an
appropriate dose of an immediate-release analgesic. If the level of pain
increases after dosage stabilization, attempt to identify the source of
increased pain before increasing the methadone hydrochloride tablets dosage.
Because of individual variability in the pharmacokinetic profile (i.e.,
terminal half-life (T1/2) from 8 to 59 hours in different studies [see Clinical Pharmacology (12.3)], titrate methadone hydrochloride tablets slowly,
with dose increases no more frequent than every 3 to 5 days. However, because
of this high variability, some patients may require substantially longer
periods between dose increases (up to 12 days). Monitor patients closely for
the development of potentially life-threatening adverse reactions (e.g., CNS
and respiratory depression).
If unacceptable opioid-related adverse reactions are observed, the subsequent doses may be reduced and/or the dosing interval adjusted (i.e., every 8 hours or every 12 hours). Adjust the dose to obtain an appropriate balance between management of pain and opioid-related adverse reactions.
2.4 Discontinuation of Methadone Hydrochloride Tablets, USP for Pain
When a patient no longer requires therapy with methadone hydrochloride tablets for pain, taper the dose gradually, by 15% to 50% every two to four days, to prevent signs and symptoms of withdrawal. If the patient develops these signs or symptoms, raise the dose to the previous level and taper more slowly, either by increasing the interval between decreases, decreasing the amount of change in dose, or both. Do not abruptly discontinue Methadone Hydrochloride Tablets, USP [see Warnings and Precautions (5.14), Drug Abuse and Dependence (9.3)].
2.5 Induction/Initial Dosing for Detoxification and Maintenance Treatment
of Opioid Addiction
|
For detoxification and maintenance of opioid dependence, methadone should be administered in accordance with the treatment standards cited in 42 CFR Section 8.12, including limitations on unsupervised administration. |
Administer the initial methadone dose under supervision, when there are no signs of sedation or intoxication, and the patient shows symptoms of withdrawal. An initial single dose of 20 to 30 mg of methadone hydrochloride tablets will often be sufficient to suppress withdrawal symptoms. The initial dose should not exceed 30 mg.
To make same-day dosing adjustments, have the patient wait 2 to 4 hours for further evaluation, when peak levels have been reached. Provide an additional 5 to 10 mg of methadone hydrochloride tablets if withdrawal symptoms have not been suppressed or if symptoms reappear.
The total daily dose of Methadone Hydrochloride tablets on the first day of treatment should not ordinarily exceed 40 mg. Adjust the dose over the first week of treatment based on control of withdrawal symptoms at the time of expected peak activity (e.g., 2 to 4 hours after dosing). When adjusting the dose, keep in mind that methadone levels will accumulate over the first several days of dosing; deaths have occurred in early treatment due to the cumulative effects. Instruct patients that the dose will “hold” for a longer period of time as tissue stores of methadone accumulate.
Use lower initial doses for patients whose tolerance is expected to be low at treatment entry. Any patient who has not taken opioids for more than 5 days may no longer be tolerant. Do not determine initial doses based on previous treatment episodes or dollars spent per day on illicit drug use.
During the induction phase of methadone maintenance treatment, patients are being withdrawn from opioids and may have opioid withdrawal symptoms. Monitor patients for signs and symptoms of opioid withdrawal including: lacrimation, rhinorrhea, sneezing, yawning, excessive perspiration, goose-flesh, fever, chilling alternating with flushing, restlessness, irritability, weakness, anxiety, depression, dilated pupils, tremors, tachycardia, abdominal cramps, body aches, involuntary twitching and kicking movements, anorexia, nausea, vomiting, diarrhea, intestinal spasms, and weight loss and consider dose adjustment as indicated.
Short-term Detoxification
For a brief course of stabilization followed by a period of medically
supervised withdrawal, titrate the patient to a total daily dose of about 40
mg in divided doses to achieve an adequate stabilizing level. After 2 to 3
days of stabilization, gradually decrease the dose of Methadone Hydrochloride
tablets. Decrease the dose of Methadone Hydrochloride tablets on a daily basis
or at 2-day intervals, keeping the amount of Methadone Hydrochloride tablets
sufficient to keep withdrawal symptoms at a tolerable level. Hospitalized
patients may tolerate a daily reduction of 20% of the total daily dose.
Ambulatory patients may need a slower schedule.
2.6 Titration and Maintenance Treatment of Opioid Dependence
Titrate patients in maintenance treatment to a dose that prevents opioid withdrawal symptoms for 24 hours, reduces drug hunger or craving, and blocks or attenuates the euphoric effects of self-administered opioids, ensuring that the patient is tolerant to the sedative effects of methadone. Most commonly, clinical stability is achieved at doses between 80 to 120 mg/day. During prolonged administration of methadone, monitor patients for persistent constipation and manage accordingly.
2.7 Medically Supervised Withdrawal after a Period of Maintenance Treatment
for Opioid Addiction
There is considerable variability in the appropriate rate of methadone taper in patients choosing medically supervised withdrawal from methadone treatment. Dose reductions should generally be less than 10% of the established tolerance or maintenance dose, and 10 to 14-day intervals should elapse between dose reductions. Apprise patients of the high risk of relapse to illicit drug use associated with discontinuation of methadone maintenance treatment.
2.8 Risk of Relapse in Patients on Methadone Maintenance Treatment of
Opioid Addiction
Abrupt opioid discontinuation can lead to development of opioid withdrawal symptoms [see Drug Abuse and Dependence (9.3)]. Opioid withdrawal symptoms have been associated with an increased risk of relapse to illicit drug use in susceptible patients.
2.9 Considerations for Management of Acute Pain during Methadone
Maintenance Treatment
Patients in methadone maintenance treatment for opioid dependence who experience physical trauma, postoperative pain or other acute pain cannot be expected to derive analgesia from their existing dose of methadone. Such patients should be administered analgesics, including opioids, in doses that would otherwise be indicated for non-methadone-treated patients with similar painful conditions. When opioids are required for management of acute pain in methadone maintenance patients, somewhat higher and/or more frequent doses will often be required than would be the case for non-tolerant patients due to the opioid tolerance induced by methadone.
2.10 Dosage Adjustment during Pregnancy
Methadone clearance may be increased during pregnancy. During pregnancy, a woman’s methadone dose may need to be increased or the dosing interval decreased. Methadone should be used in pregnancy only if the potential benefit justifies the potential risk to the fetus [see Use in Specific Populations (8.1)].
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis:
The results of carcinogenicity assessment in B6C2F1 mice and Fischer 344 rats
following dietary administration of two doses of methadone HCl have been
published. Mice consumed 15 mg/kg/day or 60 mg/kg/day methadone for two years.
These doses were approximately 0.6 and 2.5 times a human daily oral dose of
120 mg/day on a body surface area basis (HDD). There was a significant
increase in pituitary adenomas in female mice treated with 15 mg/kg/day but
not with 60 mg/kg/day. Under the conditions of the assay, there was no clear
evidence for a treatment- related increase in the incidence of neoplasms in
male rats. Due to decreased food consumption in males at the high dose, male
rats consumed 16 mg/kg/day and 28 mg/kg/day of methadone for two years. These
doses were approximately 1.3 and 2.3 times the HDD. In contrast, female rats
consumed 46 mg/kg/day or 88 mg/kg/day for two years. These doses were
approximately 3.7 and 7.1 times the HDD. Under the conditions of the assay,
there was no clear evidence for a treatment-related increase in the incidence
of neoplasms in either male or female rats.
Mutagenesis:
There are several published reports on the potential genetic toxicity of
methadone. Methadone tested positive in the in vivo mouse dominant lethal
assay and the in vivo mammalian spermatogonial chromosome aberration test.
Additionally, methadone tested positive in the E. coli DNA repair system and
Neurospora crassa and mouse lymphoma forward mutation assays. In contrast,
methadone tested negative in tests for chromosome breakage and disjunction and
sex-linked recessive lethal gene mutations in germ cells of Drosophila using
feeding and injection procedures.
Impairment of Fertility:
Published animal studies show that methadone treatment of males can alter
reproductive function. Methadone produces decreased sexual activity (mating)
of male rats at 10 mg/kg/day (corresponding to 0.3 times the human daily oral
dose of 120 mg/day based on body surface area). Methadone also produces a
significant regression of sex accessory organs and testes of male mice and
rats at 0.2 and 0.8 times the HDD, respectively. Methadone treatment of
pregnant rats from Gestation Day 14 to 19 reduced fetal blood testosterone and
androstenedione in males. Decreased serum levels of testosterone were observed
in male rats that were treated with methadone (1.3 to 3.3 mg/kg/day for 14
days, corresponding to 0.1 to 0.3 times the HDD) or 10 to 15 mg/kg/day for 10
days (0.8 to 1.2 times the HDD).
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 Storage and Handling
Methadone hydrochloride tablets, USP contains methadone which is a controlled substance. Like fentanyl, morphine, oxycodone, hydromorphone, and oxymorphone, methadone is controlled under Schedule II of the Federal Controlled Substances Act. Methadone hydrochloride tablets, USP may be targeted for theft and diversion by criminals [see Warnings and Precautions (5.1)].
Dispense in a tight, light-resistant container as defined in the USP/NF.
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature].
16.2 How Supplied
Methadone Hydrochloride Tablets, USP
10 mg tablets: white, round, biconvex tablet, scored on one side and debossed
“ASC 116” on the other side.
55700-882-30
55700-882-60
55700-882-90
55700-882-01
DEA order form required.