
SEGLENTIS
These highlights do not include all the information needed to use SEGLENTIS safely and effectively. See full prescribing information for SEGLENTIS. SEGLENTIS (celecoxib and tramadol hydrochloride) tablets, for oral use, C-IV Initial U.S. Approval: 2021
cf2c8436-a9f3-473c-e053-2a95a90a1123
HUMAN PRESCRIPTION DRUG LABEL
Mar 5, 2024
Kowa Pharmaceuticals America, Inc.
DUNS: 119459589
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
celecoxib and tramadol hydrochloride
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (11)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
PRINCIPAL DISPLAY PANEL - 56 mg / 44 mg Tablet Bottle Label
NDC 66869-564-35
SEGLENTIS
CIV
(celecoxib and tramadol
hydrochloride) tablets
For Oral Use
56 mg / 44 mg
Rx only | 35 tablets
BOXED WARNING SECTION
WARNING: SERIOUS AND LIFE-THREATENING RISKS FROM USE OF SEGLENTIS
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
SEGLENTIS is indicated for the management of acute pain in adults that is severe enough to require an opioid analgesic and for which alternative treatments are inadequate.
Limitations of Use
Because of the risks of addiction, abuse, and misuse with opioids, which can occur at any dosage or duration [see Warnings and Precautions (5.1)], reserve SEGLENTIS for use in patients for whom alternative treatment options [e.g., non-opioid analgesics]:
- Have not been tolerated or are not expected to be tolerated,
- Have not provided adequate analgesia or are not expected to provide adequate analgesia.
SEGLENTIS should not be used for an extended period of time unless the pain remains severe enough to require an opioid analgesic and for which alternative treatment options continue to be inadequate.
SEGLENTIS contains tramadol hydrochloride, an opioid agonist, and celecoxib, a nonsteroidal anti-inflammatory drug, and is indicated for the management of acute pain in adults that is severe enough to require an opioid analgesic and for which alternative treatments are inadequate (1).
Limitations of Use (1):
Because of the risks of addiction, abuse, and misuse with opioids, which can occur at any dosage or duration (5.1), reserve SEGLENTIS for use in patients for whom alternative treatment options [e.g., non-opioid analgesics]:
- Have not been tolerated or are not expected to be tolerated,
- Have not provided adequate analgesia or are not expected to provide adequate analgesia.
SEGLENTIS should not be used for an extended period of time unless the pain remains severe enough to require an opioid analgesic and for which alternative treatment options continue to be inadequate.
CONTRAINDICATIONS SECTION
4 CONTRAINDICATIONS
SEGLENTIS is contraindicated in:
- All patients younger than 12 years of age [see Warnings and Precautions (5.8)].
- Post-operative management in children younger than 18 years of age following tonsillectomy and/or adenoidectomy [see Warnings and Precautions (5.8)].
SEGLENTIS is also contraindicated in patients with:
- Significant respiratory depression [see Warnings and Precautions (5.2)].
- In the setting of coronary artery bypass graft (CABG) surgery [see Warnings and Precautions (5.6)].
- Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment [see Warnings and Precautions (5.14)].
- Known or suspected gastrointestinal obstruction, including paralytic ileus [see Warnings and Precautions (5.18)].
- Previous hypersensitivity (e.g., anaphylactic reactions and serious skin reactions) to tramadol, opioids, celecoxib, sulfonamides, or any other component of the drug product [see Warnings and Precautions (5.19)].
- Concurrent use of monoamine oxidase inhibitors (MAOIs) or use of MAOIs within the last 14 days [see Drug Interactions (7)].
- History of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs. Severe, sometimes fatal, anaphylactic reactions to NSAIDs, have been reported in such patients [see Warnings and Precautions (5.19, 5.24)].
- Children younger than 12 years of age (4).
- Postoperative management in children younger than 18 years of age following tonsillectomy and/or adenoidectomy (4).
- Significant respiratory depression (4).
- In the setting of CABG surgery (4).
- Acute or severe bronchial asthma in an unmonitored setting or in absence of resuscitative equipment (4).
- Known or suspected gastrointestinal obstruction, including paralytic ileus (4).
- Hypersensitivity to tramadol, celecoxib, any other component of this product, or sulfonamides, or opioids (4).
- Concurrent use of monoamine oxidase inhibitors (MAOIs) or use of MAOIs within the last 14 days (4).
- History of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs (4).
ADVERSE REACTIONS SECTION
6 ADVERSE REACTIONS
The following serious adverse reactions are discussed, or described in greater detail, in other sections:
- Addiction, Abuse, and Misuse [see Warnings and Precautions (5.1)]
- Life-Threatening Respiratory Depression [see Warnings and Precautions (5.2)]
- Interactions with Benzodiazepines or Other CNS Depressants [see Warnings and Precautions (5.3)]
- Neonatal Opioid Withdrawal Syndrome [see Warnings and Precautions (5.4)]
- Cardiovascular Thrombotic Events [see Warnings and Precautions (5.6)]
- Gastrointestinal Bleeding, Ulceration, and Perforation [see Warnings and Precautions (5.7)]
- Ultra-Rapid Metabolism of Tramadol and Other Risk Factors for Life-threatening Respiratory Depression in Children [see Warnings and Precautions (5.8)]
- Opioid-Induced Hyperalgesia and Allodynia [see Warnings and Precautions (5.10)]
- Serotonin Syndrome [see Warnings and Precautions (5.11)]
- Seizures [see Warnings and Precautions (5.12)]
- Suicide [see Warnings and Precautions (5.13)]
- Adrenal Insufficiency [see Warnings and Precautions (5.15)]
- Severe Hypotension [see Warnings and Precautions (5.16)]
- Gastrointestinal Adverse Reactions [see Warnings and Precautions (5.18)]
- Anaphylaxis and Other Hypersensitivity Reactions [see Warnings and Precautions (5.19)]
- Hepatotoxicity [see Warnings and Precautions (5.20)]
- Hypertension [see Warnings and Precautions (5.21)]
- Heart Failure and Edema [see Warnings and Precautions (5.22)]
- Renal Toxicity and Hyperkalemia [see Warnings and Precautions (5.23)]
- Serious Skin Reactions [see Warnings and Precautions (5.25)]
- Hematologic Toxicity [see Warnings and Precautions (5.28)]
- Withdrawal [see Warnings and Precautions (5.29)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
A total of 550 subjects in 7 clinical studies, from Phase 1 to Phase 3, were exposed to SEGLENTIS during the clinical development program, including 385 subjects exposed to 200 mg of SEGLENTIS, either single or multiple administration.
In a placebo-controlled post-bunionectomy acute pain trial, 637 patients received 200 mg of SEGLENTIS every 12 hours or 50 mg tramadol every 6 hours or 100 mg celecoxib every 12 hours or placebo, orally for 48 hours (blinded period) [see Clinical Studies (14)] and followed up to 7 days post-dose. Table 1 lists the adverse reactions reported by > 5% of patients in any treatment group and greater in SEGLENTIS than placebo. Discontinuation due to adverse events occurred in 1.6% of SEGLENTIS-treated patients (3 out of 183), 1.6% of tramadol-treated patients (3 out of 183), no celecoxib-treated patients, and no placebo-treated patients. The adverse reactions that led to discontinuation of study drug were nausea (1.1%) and pruritus/rash (0.5%) in the SEGLENTIS group, and vomiting (1.1%) and supraventricular tachycardia (0.5%) in the tramadol group.
Table 1: Reported Adverse Reactions in >5% of Patients in Any Treatment Group and greater in SEGLENTIS than Placebo|
System Organ Class |
SEGLENTIS |
Tramadol |
Celecoxib |
Placebo |
|---|---|---|---|---|
|
Total daily dose: 400 mg of SEGLENTIS (200 mg twice a day); 200 mg of tramadol
(50 mg four times a day); 200 mg of celecoxib (100 mg twice a day); or
placebo. | ||||
|
Gastrointestinal disorders | ||||
|
Nausea |
55 (30.1) |
69 (37.7) |
30 (16.5) |
17 (19.1) |
|
Vomiting |
29 (15.8) |
30 (16.4) |
4 (2.2) |
2 (2.2) |
|
Nervous system disorders | ||||
|
Dizziness |
31 (16.9) |
34 (18.6) |
9 (4.9) |
13 (14.6) |
|
Headache |
21 (11.5) |
33 (18.0) |
20 (11.0) |
6 (6.7) |
|
Somnolence |
15 (8.2) |
10 (5.5) |
4 (2.2) |
3 (3.4) |
|
Metabolism and nutritional disorders | ||||
|
Decreased appetite |
6 (3.3) |
11 (6.0) |
1 (0.5) |
0 |
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of either tramadol or celecoxib-containing products. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Serotonin Syndrome
Cases of serotonin syndrome, a potentially life-threatening condition, have been reported during concomitant use of opioids with serotonergic drugs.
Adrenal Insufficiency
Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use.
Androgen Deficiency
Cases of androgen deficiency have occurred with use of opioids for an extended period of time [see Clinical Pharmacology (12.2)].
QT Prolongation/Torsade De Pointes
Cases of QT prolongation and/or torsade de pointes have been reported with tramadol use. Many of these cases were reported in patients taking another drug labeled for QT prolongation, in patients with a risk factor for QT prolongation (e.g., hypokalemia), or in the overdose setting.
Eye Disorders
Miosis, mydriasis.
Metabolism and Nutrition Disorders
Cases of hypoglycemia have been reported very rarely in patients taking tramadol. Most reports were in patients with predisposing risk factors, including diabetes or renal insufficiency, or in elderly patients.
Hyponatremia
Cases of severe hyponatremia and/or SIADH have been reported in patients taking tramadol, most often in females over the age of 65, and within the first week of therapy [see Warnings and Precautions (5.32)].
Hypoglycemia
Cases of hypoglycemia have been reported in patients taking tramadol. Most reports were in patients with predisposing risk factors, including diabetes or renal insufficiency, or in elderly patients [see Warnings and Precautions (5.33)].
Opioid-Induced Hyperalgesia and Allodynia
Cases of hyperalgesia and allodynia have been reported with opioid therapy of any duration [see Warnings and Precautions (5.10)].
Nervous System Disorders
Movement disorder, speech disorder.
Psychiatric Disorders
Delirium.
Cardiovascular
Vasculitis, deep venous thrombosis.
General
Anaphylactoid reaction, angioedema.
Liver and Biliary
Liver necrosis, hepatitis, jaundice, hepatic failure.
Hemic and Lymphatic
Agranulocytosis, aplastic anemia, pancytopenia, leucopenia.
Metabolic
Hypoglycemia, hyponatremia.
Nervous
Aseptic meningitis, ageusia, anosmia, fatal intracranial hemorrhage.
Renal
Interstitial nephritis.
Most common adverse reactions (incidence > 5% and > placebo) are nausea, vomiting, dizziness, headache, somnolence (6.1).
To report SUSPECTED ADVERSE REACTIONS, contact Kowa Pharmaceuticals America, Inc., at toll-free phone 1-888-SEGLENTIS or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DOSAGE FORMS & STRENGTHS SECTION
3 DOSAGE FORMS AND STRENGTHS
SEGLENTIS coated tablets contain 56 mg celecoxib and 44 mg tramadol hydrochloride (equivalent to 39 mg tramadol). The tablets are white to off- white elongated coated tablets debossed with "100" on one side and "CTC" on the other.
Tablet: celecoxib 56 mg and tramadol hydrochloride 44 mg (3).
DRUG ABUSE AND DEPENDENCE SECTION
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
SEGLENTIS contains tramadol, a Schedule IV controlled substance.
9.2 Abuse
SEGLENTIS contains tramadol, a substance with high potential for misuse and abuse, which can lead to the development of substance use disorder, including addiction [see Warnings and Precautions (5.1)].
Misuse is the intentional use, for therapeutic purposes, of a drug by an individual in a way other than prescribed by a healthcare provider or for whom it was not prescribed.
Abuse is the intentional, non-therapeutic use of a drug, even once, for its desirable psychological or physiological effects.
Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that may include a strong desire to take the drug, difficulties in controlling drug use, (e.g., continuing drug use despite harmful consequences, giving a higher priority to drug use than other activities and obligations), and possible tolerance or physical dependence.
Misuse and abuse of SEGLENTIS increases risk of overdose, which may lead to central nervous system and respiratory depression, hypotension, seizures, and death. The risk is increased with concurrent use of SEGLENTIS with alcohol and/or other CNS depressants. Abuse and addiction to opioids may not be accompanied by concurrent tolerance and symptoms of physical dependence. In addition, abuse of opioids can occur in the absence of addiction.
All patients treated with opioids require careful and frequent reevaluation for signs of misuse, abuse, and addiction, because use of opioid analgesic products carries the risk of addiction even under appropriate medical use. Patients at high risk of SEGLENTIS abuse include those with a history of prolonged use of any opioid, including products containing tramadol, those with a history of drug or alcohol abuse, or those who use SEGLENTIS in combination with other abused drugs.
"Drug seeking" behavior is very common in persons with substance use disorders. Drug seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing or referral, repeated "loss" of prescriptions, tampering with prescriptions, and reluctance to provide prior medical records or contact information for other treating healthcare provider(s). "Doctor shopping" (visiting multiple prescribers to obtain additional prescriptions) is common among people who abuse drugs and people with substance use disorder. Preoccupation with achieving adequate pain relief can be appropriate behavior in a patient with inadequate pain control.
SEGLENTIS, like other opioids, can be diverted for nonmedical use into illicit channels of distribution. Careful record-keeping of prescribing information, including quantity, frequency, and renewal requests, as required by state and federal law, is strongly advised.
Proper assessment of the patient, proper prescribing practices, periodic reevaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs.
Risks Specific to Abuse of SEGLENTIS
Abuse of SEGLENTIS poses a risk of overdose and death. The risk is increased with concurrent use of SEGLENTIS with alcohol and/or other CNS depressants.
SEGLENTIS is approved for oral use only.
Parenteral drug abuse is commonly associated with transmission of infectious diseases such as hepatitis and HIV.
9.3 Dependence
Both tolerance and physical dependence can develop during use of opioid therapy.
Tolerance is a physiological state characterized by a reduced response to a drug after repeated administration (i.e., higher dose of a drug is required to produce the same effect that was once obtained at a lower dose).
Physical dependence is a state that develops as a result of a physiological adaptation in response to repeated drug use, manifested by withdrawal signs and symptoms after abrupt discontinuation or a significant dose reduction of a drug.
Withdrawal may be precipitated through the administration of drugs with opioid antagonist activity (e.g., naloxone), mixed agonist/antagonist analgesics (e.g., pentazocine, butorphanol, nalbuphine), or partial agonists (e.g., buprenorphine). Physical dependence may not occur to a clinically significant degree until after several days to weeks of continued use.
Do not abruptly discontinue SEGLENTIS in a patient physically dependent on opioids. Rapid tapering of SEGLENTIS in a patient physically dependent on opioids may lead to serious withdrawal symptoms, uncontrolled pain, and suicide. Rapid discontinuation has also been associated with attempts to find other sources of opioid analgesics, which may be confused with drug-seeking for abuse.
When discontinuing SEGLENTIS, gradually taper the dosage using a patient- specific plan that considers the following: the dose of SEGLENTIS the patient has been taking, the duration of treatment, and the physical and psychological attributes of the patient. To improve the likelihood of a successful taper and minimize withdrawal symptoms, it is important that the opioid tapering schedule is agreed upon by the patient. In patients taking opioids for an extended period of time at high doses, ensure that a multimodal approach to pain management, including mental health support (if needed), is in place prior to initiating an opioid analgesic taper [see Dosage and Administration (2.4), Warnings and Precautions (5.29)]. If SEGLENTIS is abruptly discontinued in a physically-dependent patient, a withdrawal syndrome may occur. Some or all of the following can characterize this syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, myalgia, and mydriasis. Other signs and symptoms also may develop, including irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, or increased blood pressure, respiratory rate, or heart rate.
Infants born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal signs [see Use in Specific Populations (8.1)].
OVERDOSAGE SECTION
10 OVERDOSAGE
Clinical Presentation
SEGLENTIS is a combination drug composed of tramadol and celecoxib. The clinical presentation of overdose may include the signs and symptoms of tramadol toxicity, celecoxib toxicity or both.
Tramadol
Acute overdose with tramadol can be manifested by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, and, in some cases, pulmonary edema, bradycardia, QT prolongation, hypotension, partial or complete airway obstruction, atypical snoring, seizures, and death. Marked mydriasis rather than miosis may be seen with hypoxia in overdose situations.
Deaths due to overdose have been reported with abuse and misuse of tramadol [see Warnings and Precautions (5.1); Drug Abuse and Dependence (9.2)]. Review of case reports has indicated that the risk of fatal overdose is further increased when tramadol is abused concurrently with alcohol or other CNS depressants, including other opioids.
Celecoxib
Symptoms following acute NSAID overdosages have been typically limited to lethargy, drowsiness, nausea, vomiting, and epigastric pain, which have been generally reversible with supportive care. Gastrointestinal bleeding has occurred. Hypertension, acute renal failure, respiratory depression, and coma have occurred, but were rare [see Warnings and Precautions (5.6, 5.7, 5.21, 5.23)].
No overdoses of celecoxib were reported during clinical trials. Doses up to 2400 mg/day for up to 10 days in 12 patients did not result in serious toxicity. No information is available regarding the removal of celecoxib by hemodialysis but based on its high degree of plasma protein binding (>97%) dialysis is unlikely to be useful in overdose.
Treatment of Overdose
Tramadol
In case of overdose, priorities are the re-establishment of a patent and protected airway and institution of assisted or controlled ventilation, if needed. Employ other supportive measures (including oxygen and vasopressors) in the management of circulatory shock and pulmonary edema as indicated. Cardiac arrest or arrhythmias will require advanced life-supporting measures.
Opioid antagonists, such as naloxone, are specific antidotes to respiratory depression resulting from opioid overdose. For clinically significant respiratory or circulatory depression secondary to tramadol overdose, administer an opioid antagonist.
While naloxone will reverse some, but not all, symptoms caused by overdosage with tramadol, the risk of seizures is also increased with naloxone administration. In animals, convulsions following the administration of toxic doses of tramadol could be suppressed with barbiturates or benzodiazepines but were increased with naloxone.
Naloxone administration did not change the lethality of an overdose in mice. Hemodialysis is not expected to be helpful in an overdose because it removes less than 7% of the administered dose in a 4-hour dialysis period.
Because the duration of opioid reversal is expected to be less than the duration of action of tramadol in SEGLENTIS, carefully monitor the patient until spontaneous respiration is reliably re-established. If the response to an opioid antagonist is suboptimal or only brief in nature, administer additional antagonist as directed by the product's prescribing information.
In an individual physically dependent on opioids, administration of the recommended usual dosage of the antagonist will precipitate an acute withdrawal syndrome. The severity of the withdrawal symptoms experienced will depend on the degree of physical dependence and the dose of the antagonist administered. If a decision is made to treat serious respiratory depression in the physically dependent patient, administration of the antagonist should be begun with care and by titration with smaller than usual doses of the antagonist.
Celecoxib
Manage patients with symptomatic and supportive care following an NSAID overdosage. There are no specific antidotes. Consider emesis and/or activated charcoal (60 to 100 grams in adults, 1 to 2 grams per kg of body weight in pediatric patients) and/or osmotic cathartic in symptomatic patients seen within four hours of ingestion or in patients with a large overdosage (5 to 10 times the recommended dosage). Forced diuresis, alkalinization of urine, hemodialysis, or hemoperfusion may not be useful due to high protein binding.
For additional information about overdosage treatment contact a poison control center (1-800-222-1222).
DESCRIPTION SECTION
11 DESCRIPTION
SEGLENTIS (celecoxib and tramadol hydrochloride) tablets contains a co-crystal with molecular weight of 681.2, composed of tramadol hydrochloride, an analgesic and opioid agonist, and celecoxib, a nonsteroidal anti-inflammatory drug, in a 1:1 molecular ratio.
The chemical name for tramadol hydrochloride is (1RS,2RS)-2-[(dimethylamino)methyl]-1-(3-methoxyphenyl)cyclohexanol hydrochloride (C16H26ClNO2). The structural formula is:
The molecular weight of tramadol hydrochloride is 299.84 (the molecular weight of tramadol is 263.38).
The chemical name for celecoxib is 4-[5-(4-methylphenyl)-3-(trifluoromethyl)-1H-pyrazol-1-yl] benzenesulfonamide and is a diaryl-substituted pyrazole (C17H14F3N3O2S). The molecular weight is 381.38 and it has the following chemical structure:
SEGLENTIS coated tablets contain 56 mg celecoxib and 44 mg of tramadol hydrochloride (equivalent to 39 mg tramadol) in a co-crystal structure. Tablets are white to off-white in color. Inactive ingredients in the tablet are sodium lauryl sulfate, crospovidone, mannitol, sodium stearyl fumarate, talc, cellulose microcrystalline, copovidone and color mixture (polyvinyl alcohol partially hydrolyzed, titanium dioxide, polyethylene glycol and talc).
INFORMATION FOR PATIENTS SECTION
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Storage and Disposal
Because of the risks associated with accidental ingestion, misuse, and abuse, advise patients to store SEGLENTIS securely, out of sight and reach of children, and in a location not accessible by others, including visitors to the home. Inform patients that leaving SEGLENTIS unsecured can pose a deadly risk to others in the home [see Warnings and Precautions (5.1, 5.2), Drug Abuse and Dependence (9.2)].
Advise patients and caregivers that when medicines are no longer needed, they should be disposed of promptly. Inform patients that medicine take-back options are the preferred way to safely dispose of most types of unneeded medicines. If no take back programs or Drug Enforcement Administration (DEA)-registered collectors are available, instruct patients to dispose of SEGLENTIS by following these four steps:
- Mix SEGLENTIS (do not crush) with an unpalatable substance such as dirt, cat litter, or used coffee grounds;
- Place the mixture in a container such as a sealed plastic bag;
- Throw the container in the household trash;
- Remove all personal information on the prescription label of the empty bottle.
Inform patients that they can visit www.fda.gov/drugdisposal for additional information on disposal of unused medicines.
Addiction, Abuse, and Misuse
Inform patients that the use of SEGLENTIS, even when taken as recommended, can result in addiction, abuse, and misuse, which can lead to overdose and death [see Warnings and Precautions (5.1)]. Instruct patients not to share SEGLENTIS with others and to take steps to protect SEGLENTIS from theft or misuse.
Life-Threatening Respiratory Depression
Inform patients of the risk of life-threatening respiratory depression, including information that the risk is greatest when starting SEGLENTIS or when the dosage is increased, and that it can occur even at recommended dosages [see Warnings and Precautions (5.2)].
Educate patients and caregivers on how to recognize respiratory depression and emphasize the importance of calling 911 or getting emergency medical help right away in the event of a known or suspected overdose [see Warnings and Precautions (5.2)].
Accidental Ingestion
Inform patients that accidental ingestion, especially by children, may result in respiratory depression or death [see Warnings and Precautions (5.3)]. Instruct patients to take steps to store SEGLENTIS securely and to dispose of unused SEGLENTIS in accordance with the local state guidelines and/or regulations.
Interactions with Benzodiazepines and Other CNS Depressants
Inform patients and caregivers that potentially fatal additive effects may occur if SEGLENTIS is used with benzodiazepines, CNS depressants, including alcohol, or some illicit drugs and not to use these concomitantly unless supervised by a healthcare provider [see Warnings and Precautions (5.9); Drug Interactions (7)].
Patient Access to Naloxone for the Emergency Treatment of Opioid Overdose
Discuss with the patient and caregiver the availability of naloxone for the emergency treatment of opioid overdose, both when initiating and renewing treatment with SEGLENTIS. Inform patients and caregivers about the various ways to obtain naloxone as permitted by individual state naloxone dispensing and prescribing requirements or guidelines (e.g., by prescription, directly from a pharmacist, or as part of a community-based program) [see Dosage and Administration (2.2), Warnings and Precautions (5.2)].
Educate patients and caregivers on how to recognize the signs and symptoms of an overdose.
Explain to patients and caregivers that naloxone's effects are temporary, and that they must call 911 or get emergency medical help right away in all cases of known or suspected opioid overdose, even if naloxone is administered [see Overdosage (10)].
If naloxone is prescribed, also advise patients and caregivers:
- How to treat with naloxone in the event of an opioid overdose
- To tell family and friends about their naloxone and to keep it in a place where family and friends can access it in an emergency
- To read the Patient Information (or other educational material) that will come with their naloxone. Emphasize the importance of doing this before an opioid emergency happens, so the patient and caregiver know what to do.
Cardiovascular Thrombotic Events
Advise patients to be alert for the symptoms of cardiovascular thrombotic events, including chest pain, shortness of breath, weakness, or slurring of speech, and to report any of these symptoms to their health care provider immediately [see Warnings and Precautions (5.6)].
Gastrointestinal Bleeding, Ulceration, and Perforation
Advise patients to report symptoms of ulcerations and bleeding, including epigastric pain, dyspepsia, melena, and hematemesis to their health care provider. In the setting of concomitant use of low-dose aspirin for cardiac prophylaxis, inform patients of the increased risk for and the signs and symptoms of GI bleeding [see Warnings and Precautions (5.7)].
Ultra-Rapid Metabolism of Tramadol and Other Risk Factors for Life-threatening Respiratory Depression in Children
Advise caregivers that SEGLENTIS is contraindicated in children younger than 12 years of age and in children younger than 18 years of age following tonsillectomy and/or adenoidectomy. Advise caregivers of children ages 12 to 18 years of age receiving SEGLENTIS to watch for signs of respiratory depression [see Warnings and Precautions (5.8)].
Opioid-Induced Hyperalgesia and Allodynia
Inform patients and caregivers not to increase opioid dosage without first consulting a clinician. Advise patients to seek medical attention if they experience symptoms of hyperalgesia, including worsening pain, increased sensitivity to pain, or new pain. Inform patients and caregivers not to exceed the recommended dose of SEGLENTIS [see Warnings and Precautions (5.10), Adverse Reactions (6.2)].
Serotonin Syndrome
Inform patients that opioids could cause a rare but potentially life- threatening condition called serotonin syndrome resulting from concomitant administration of serotonergic drugs. Warn patients of the symptoms of serotonin syndrome, and to seek medical attention right away if symptoms develop. Instruct patients to inform their healthcare provider if they are taking, or plan to take serotonergic medications [see Warnings and Precautions (5.11), Drug Interactions (7)].
Seizures
Inform patients that SEGLENTIS may cause seizures with concomitant use of serotonergic agents (including SSRIs, SNRIs, and triptans) or drugs that significantly reduce the metabolic clearance of tramadol [see Warnings and Precautions (5.12)].
MAOI Interaction
Inform patients not to take SEGLENTIS while using any drugs that inhibit monoamine oxidase. Patients should not start MAOIs while taking SEGLENTIS [see Drug Interactions (7)].
Important Administration Instructions
- Instruct patients how to properly take SEGLENTIS [see Dosage and Administration (2)].
- Advise patients not to modify the dose of SEGLENTIS without consulting with a physician or other healthcare professional.
- If patients have been receiving treatment with SEGLENTIS for more than a few weeks and cessation of therapy is indicated, counsel them on the importance of safely tapering the dose as abrupt discontinuation of the medication could precipitate withdrawal symptoms. Provide a dose schedule to accomplish a gradual discontinuation of the medication [see Dosage and Administration (2.4)].
Maximum single-dose and 24-hour dose
Advise patients not to exceed the single-dose and 24-hour dose limit and the time interval between doses, since exceeding these recommendations can result in respiratory depression, seizures, and death [see Dosage and Administration (2); Warnings and Precautions (5.2)].
Driving or Operating Heavy Machinery
Advise patients that SEGLENTIS may impair the ability to perform potentially hazardous activities such as driving a car or operating heavy machinery. Advise patients not to perform such tasks until they know how they will react to the medication [see Warnings and Precautions (5.30)].
Constipation
Advise patients of the potential for severe constipation, including management instructions and when to seek medical attention [see Adverse Reactions (6)].
Adrenal Insufficiency
Inform patients that opioids could cause adrenal insufficiency, a potentially life-threatening condition. Adrenal insufficiency may present with non- specific symptoms and signs such as nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. Advise patients to seek medical attention if they experience a constellation of these symptoms [see Warnings and Precautions (5.15)].
Hypotension
Inform patients that SEGLENTIS may cause orthostatic hypotension and syncope. Instruct patients how to recognize symptoms of low blood pressure and how to reduce the risk of serious consequences should hypotension occur (e.g., sit or lie down, carefully rise from a sitting or lying position) [see Warnings and Precautions (5.16)].
Anaphylaxis
Inform patients that anaphylaxis has been reported with ingredients contained in SEGLENTIS. Advise patients how to recognize such a reaction and when to seek medical attention.
Inform patients of the signs of an anaphylactic reaction (e.g., difficulty breathing, swelling of the face or throat). Instruct patients to seek immediate emergency help if these occur [see Contraindications (4) and Warnings and Precautions (5.19); Adverse Reactions (6)].
Hepatotoxicity
Inform patients of the warning signs and symptoms of hepatotoxicity (e.g., nausea, fatigue, lethargy, pruritus, diarrhea jaundice, right upper quadrant tenderness, and "flu-like" symptoms). If these occur, instruct patients to stop SEGLENTIS and seek immediate medical therapy [see Warnings and Precautions (5.20), Use in Specific Populations (8.6)].
Heart Failure and Edema
Advise patients to be alert for the symptoms of congestive heart failure including shortness of breath, unexplained weight gain, or edema and to contact their healthcare provider if such symptoms occur [see Warnings and Precautions (5.22)].
Serious Skin Reactions, including DRESS
Advise patients to stop taking SEGLENTIS immediately if they develop any type of rash or fever and to contact their healthcare provider as soon as possible [see Warnings and Precautions (5.25, 5.26)].
Avoid Concomitant Use of NSAIDs
Inform patients that the concomitant use of SEGLENTIS with other NSAIDs or salicylates (e.g., diflunisal, salsalate) is not recommended due to the increased risk of gastrointestinal toxicity, and little or no increase in efficacy [see Warnings and Precautions (5.7) and Drug Interactions (7)]. Alert patients that NSAIDs may be present in "over the counter" medications for treatment of colds, fever, or insomnia.
Use of NSAIDs and Low-Dose Aspirin
Inform patients not to use low-dose aspirin concomitantly with SEGLENTIS until they talk to their healthcare provider [see Drug Interactions (7)].
Pregnancy
Neonatal Opioid Withdrawal Syndrome
Inform female patients of reproductive potential that use of SEGLENTIS for an extended period of time during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated and that the patient should inform their healthcare provider if they have used opioids at any time during their pregnancy, especially near the time of birth [see Warnings and Precautions (5.4); Use in Specific Populations (8.1)].
Embryo-Fetal Toxicity
Advise female patients of reproductive potential that SEGLENTIS may cause fetal harm and to inform the healthcare provider of a known or suspected pregnancy [see Use in Specific Populations (8.1)].
Inform pregnant women to avoid use of SEGLENTIS and other NSAIDS starting at 30 weeks of gestation because of the risk of the premature closing of the fetal ductus arteriosus. If treatment with SEGLENTIS is needed for a pregnant woman between about 20 to 30 weeks gestation, advise her that she may need to be monitored for oligohydramnios, if treatment continues for longer than 48 hours [see Warnings and Precautions (5.27) and Use in Specific Populations (8.1)].
Lactation
Advise women that breastfeeding is not recommended during treatment with SEGLENTIS [see Warnings and Precautions (5.4); Use in Specific Populations (8.2)].
Infertility
Advise patients that use of opioids for an extended period of time may cause reduced fertility. It is not known whether these effects on fertility are reversible [see Use in Specific Populations (8.3)].
Advise females of reproductive potential who desire pregnancy that NSAIDs, including the celecoxib contained in SEGLENTIS, may be associated with a reversible delay in ovulation [see Use in Specific Populations (8.3)].
SPL UNCLASSIFIED SECTION
Manufactured and Packaged by:
Towa Pharmaceutical Europe, S.L.
Martorelles, 08107 Barcelona Spain
Distributed by:
Kowa Pharmaceuticals America, Inc.
Montgomery, AL 36117 USA
FPI-SEG-US-00010 12/2023
SEGLENTIS® is a registered trademark of Esteve Pharmaceuticals, S.A. and is
used under license.
© Kowa Pharmaceuticals America, Inc. (2021)
SPL MEDGUIDE SECTION
|
This Medication Guide has been approved by the U.S. Food and Drug Administration. |
Issued: 12/2023 |
|
Medication Guide | |
|
SEGLENTIS is:
| |
|
Important information about SEGLENTIS: *Get emergency help or call 911 right away if you take too much SEGLENTIS (overdose). When you first start taking SEGLENTIS, when your dose is changed, or if you take too much (overdose), serious or life-threatening breathing problems that can lead to death may occur. Talk to your healthcare provider about naloxone, a medicine for the emergency treatment of an opioid overdose.
| |
|
Important Information Guiding Use in Pediatric Patients:
| |
|
Do not take SEGLENTIS if you have:
| |
|
Do not take SEGLENTIS right before or after heart bypass surgery. | |
|
Before taking SEGLENTIS,tell your healthcare provider about all of your medical conditions, including if you have a history of:
| |
|
Tell your healthcare provider if you: *Are pregnant or plan to become pregnant: Use of SEGLENTIS for an extended period of time during pregnancy can cause withdrawal symptoms in your newborn baby that could be life-threatening if not recognized and treated. Taking SEGLENTIS at about 20 weeks of pregnancy or later may harm your unborn baby. If you need to take SEGLENTIS for more than 2 days when you are between 20 and 30 weeks of pregnancy, your healthcare provider may need to monitor the amount of fluid in your womb around your baby.You should not take SEGLENTIS and other NSAIDs after about 30 weeks of pregnancy. Tell your healthcare provider if you become pregnant or think that you may be pregnant. *Are breastfeeding: Not recommended; may harm your baby.
| |
|
When taking SEGLENTIS:
| |
|
While taking SEGLENTIS DO NOT:
| |
|
The possible side effects of SEGLENTIS:
| |
|
Get emergency medical help or call 911 right away if you have:
| |
|
Stop taking SEGLENTIS and call your healthcare provider right away if you get any of the following symptoms:
| |
|
SEGLENTIS may cause fertility problems in males and females, which may affect the ability to have children. Talk to your healthcare provider if you have concerns about fertility. | |
|
These are not all the possible side effects of SEGLENTIS. Call your doctor for medical advice about side effects. | |
|
You may report side effects to FDA at 1-800-FDA-1088.For more information go to dailymed.nlm.nih.gov. | |
|
Other information about NSAIDs:
| |
|
and intestines. Aspirin can also cause ulcers in the stomach and intestines. | |
| |
|
General information about the safe and effective use of SEGLENTIS. | |
|
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use SEGLENTIS for a condition for which it was not prescribed. Do not give SEGLENTIS to other people, even if they have the same symptoms that you have. It may harm them. | |
|
If you would like more information about SEGLENTIS, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about SEGLENTIS that is written for health professionals. | |
|
Distributed by: Kowa Pharmaceuticals America, Inc. Montgomery, AL 36117
USA. For more information, go to www.seglentisrx.com or call 1-888-SEGLENTIS. |
RECENT MAJOR CHANGES SECTION
RECENT MAJOR CHANGES
|
Boxed Warning |
12/2023 |
|
Indications and Usage (1) |
12/2023 |
|
Dosage and Administration (2.1, 2.3) |
12/2023 |
|
Warnings and Precautions (5.10) |
12/2023 |
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on animal data, advise pregnant women of the potential risk to fetus.
Use of opioid analgesics for an extended period of time during pregnancy may
cause neonatal opioid withdrawal syndrome (see Warnings and Precautions
(5.4)).
Use of NSAIDs, including SEGLENTIS, can cause premature closure of the fetal ductus arteriosus and fetal renal dysfunction leading to oligohydramnios and, in some cases, neonatal renal impairment. Because of these risks, limit dose and duration of SEGLENTIS use between about 20 and 30 weeks of gestation and avoid SEGLENTIS use at about 30 weeks of gestation and later in pregnancy (see Clinical Considerations, Data).
There are no available data on use of SEGLENTIS in pregnant women. In an animal reproduction study, oral administration of celecoxib and tramadol co- crystal to pregnant rabbits during the period of organogenesis, resulted in embryo-fetal deaths and an increase of incidence of vertebral defects at approximately 4.7 and 0.11 times the dose of celecoxib and tramadol, respectively, at the maximum recommended human dose (MRHD) of SEGLENTIS at 400 mg/day (224 mg celecoxib/176 mg tramadol) (see Data).
Tramadol
Available data with tramadol use in pregnant women are insufficient to inform a drug-associated risk for major birth defects, miscarriage, or adverse maternal outcomes. There are adverse outcomes reported with fetal exposure to opioid analgesics (see Clinical Considerations). In animal reproduction studies, tramadol administration during organogenesis decreased fetal weights and reduced ossification in mice, rats, and rabbits at 3.2, 1.4, and 8.2 times the tramadol dose of 176 mg at the MRHD of SEGLENTIS. In a pre- and post-natal development study, tramadol decreased pup body weight and increased pup mortality at 2.7 and 4.3 times the MRHD, respectively.
In a published study, tramadol caused structural abnormalities in the brains of fetuses when administered to female Sprague Dawley rats from Gestation Days 10 to 21 at 2.7 times the MRHD (see Data).
Celecoxib
Premature Closure of Fetal Ductus Arteriosus:
Use of NSAIDs, including SEGLENTIS, at about 30 weeks gestation or later in pregnancy increases the risk of premature closure of the fetal ductus arteriosus.
Oligohydramnios/Neonatal Renal Impairment:
Use of NSAIDs at about 20 weeks gestation or later in pregnancy has been associated with cases of fetal renal dysfunction leading to oligohydramnios and, in some cases, neonatal renal impairment.
Data from observational studies regarding other potential embryofetal risks of NSAID use in women in the first or second trimesters of pregnancy are inconclusive. In animal reproduction studies, embryo-fetal deaths and an increase in diaphragmatic hernias were observed in rats administered celecoxib daily during the period of organogenesis at oral doses approximately 13 times the celecoxib dose of 224 mg at the MRHD of SEGLENTIS. In addition, structural abnormalities (e.g., septal defects, ribs fused, sternebrae fused and sternebrae misshapen) were observed in rabbits given daily oral doses of celecoxib during the period of organogenesis at approximately 4 times the MRHD (see Data). Based on animal data, prostaglandins have been shown to have an important role in endometrial vascular permeability, blastocyst implantation, and decidualization. In animal studies, administration of prostaglandin synthesis inhibitors such as celecoxib, resulted in increased pre- and post- implantation loss. Prostaglandins also have been shown to have an important role in fetal kidney development. In published animal studies, prostaglandin synthesis inhibitors have been reported to impair kidney development when administered at clinically relevant doses.
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Tramadol:
Use of opioid analgesics for an extended period of time during pregnancy for medical or nonmedical purposes can result in respiratory depression and physical dependence in the neonate and neonatal opioid withdrawal syndrome shortly after birth.
Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea, and failure to gain weight. The onset, duration, and severity of neonatal opioid withdrawal syndrome vary based on the specific opioid used, duration of use, timing, and amount of last maternal use, and rate of elimination of the drug by the newborn. Observe newborns for symptoms and signs of neonatal opioid withdrawal syndrome and manage accordingly [see Warnings and Precautions (5.4)].
Neonatal seizures, neonatal withdrawal syndrome, fetal death and stillbirth have been reported with tramadol hydrochloride during postmarketing.
Celecoxib:
Premature Closure of Fetal Ductus Arteriosus:
Avoid use of NSAIDs in women at about 30 weeks gestation and later in pregnancy, because NSAIDs, including SEGLENTIS, can cause premature closure of the fetal ductus arteriosus (see Data).
Oligohydramnios/Neonatal Renal Impairment:
If an NSAID is necessary, including SEGLENTIS, at about 20 weeks gestation or later in pregnancy, limit the use to the lowest effective dose and shortest duration possible. If SEGLENTIS treatment extends beyond 48 hours, consider monitoring with ultrasound for oligohydramnios. If oligohydramnios occurs, discontinue SEGLENTIS and follow up according to clinical practice (see Data).
Labor or Delivery
Tramadol:
Opioids cross the placenta and may produce respiratory depression and psycho- physiologic effects in neonates. An opioid antagonist, such as naloxone, must be available for reversal of opioid induced respiratory depression in the neonate. SEGLENTIS is not recommended for use in pregnant women during or immediately prior to labor, when other analgesic techniques are more appropriate.
Opioid analgesics, including SEGLENTIS, can prolong labor through actions which temporarily reduce the strength, duration, and frequency of uterine contractions. However, this effect is not consistent and may be offset by an increased rate of cervical dilation, which tends to shorten labor. Monitor neonates exposed to opioid analgesics during labor for signs of excess sedation and respiratory depression.
Tramadol has been shown to cross the placenta. The mean ratio of serum tramadol in the umbilical veins compared to maternal veins was 0.83 for 40 women given tramadol during labor.
The effect of SEGLENTIS, if any, on the later growth, development, and functional maturation of the child is unknown.
Celecoxib:
There are no studies on the effects of SEGLENTIS during labor or delivery. In animal studies, NSAIDs, including celecoxib, inhibit prostaglandin synthesis, cause delayed parturition, and increase the incidence of stillbirth.
Data
Human Data
Celecoxib:
The available data do not establish the presence or absence of developmental toxicity related to the use of celecoxib.
Premature Closure of Fetal Ductus Arteriosus
Published literature reports that the use of NSAIDs at about 30 weeks of gestation and later in pregnancy may cause premature closure of the fetal ductus arteriosus.
Oligohydramnios/Neonatal Renal Impairment
Published studies and postmarketing reports describe maternal NSAID use at about 20 weeks gestation or later in pregnancy associated with fetal renal dysfunction leading to oligohydramnios, and in some cases, neonatal renal impairment. These adverse outcomes are seen, on average, after days to weeks of treatment, although oligohydramnios has been infrequently reported as soon as 48 hours after NSAID initiation. In many cases, but not all, the decrease in amniotic fluid was transient and reversible with cessation of the drug. There have been a limited number of case reports of maternal NSAID use and neonatal renal dysfunction without oligohydramnios, some of which were irreversible. Some cases of neonatal renal dysfunction required treatment with invasive procedures, such as exchange transfusion or dialysis.
Methodological limitations of these postmarketing studies and reports include lack of a control group; limited information regarding dose, duration, and timing of drug exposure; and concomitant use of other medications. These limitations preclude establishing a reliable estimate of the risk of adverse fetal and neonatal outcomes with maternal NSAID use. Because the published safety data on neonatal outcomes involved mostly preterm infants, the generalizability of certain reported risks to the full-term infant exposed to NSAIDs through maternal use is uncertain.
Animal Data
Treatment of pregnant rabbits during organogenesis with celecoxib and tramadol co-crystal resulted in an increase in the incidence of scoliosis and other vertebral defects (including absent thoracic hemicentrum/a and neural arch(es) and fused thoracic vertebral centra and/or neural arch(es)) at an oral dose of 100 mg/kg/day (56 mg celecoxib/44 mg tramadol/kg/day; approximately 4.7 and 0.11 times the MRHD on the basis of celecoxib and tramadol, respectively, on an AUC basis), which is a dose that also caused maternal toxicity (decreased body weight gain). In addition, there was a slight increase of post- implantation loss in rabbits at 100 mg/kg/day. The No Observed Adverse Effect Level (NOAEL) for embryofetal toxicity was 55 mg/kg/day (approximately 3.3 and 0.02 times the MRHD of celecoxib and tramadol, respectively, on an AUC basis).
Tramadol:
Tramadol has been shown to be embryotoxic and fetotoxic in mice, (120 mg/kg), rats (25 mg/kg) and rabbits (75 mg/kg) at maternally toxic dosages, but was not teratogenic at these dose levels. These doses on a mg/m2 basis are 3.2, 1.4, and 8.2 times the MRHD of tramadol (176 mg) for mouse, rat, and rabbit, respectively. No drug-related teratogenic effects were observed in progeny of mice (up to 140 mg/kg), rats (up to 80 mg/kg) or rabbits (up to 300 mg/kg) treated with tramadol by various routes. Embryo and fetal toxicity consisted primarily of decreased fetal weights, decreased skeletal ossification and increased supernumerary ribs at maternally toxic dose levels. Transient delays in developmental or behavioral parameters were also seen in pups from rat dams allowed to deliver. Embryo and fetal lethality were reported only in one rabbit study at 300 mg/kg, a dose that would cause extreme maternal toxicity in the rabbit. The dosages listed for mouse, rat and rabbit are 3.9, 4.3, and 33 times the MRHD of tramadol (176 mg), respectively, on a mg/m2 basis.
Tramadol was evaluated in pre-and post-natal studies in rats. Progeny of dams receiving oral (gavage) dose levels of 50 mg/kg (2.7 times the MRHD of tramadol on a mg/m2 basis) or greater had decreased weights, and pup survival was decreased early in lactation at 80 mg/kg (4.3 times the MRHD of tramadol on a mg/m2 basis).
In a published study, oral administration of tramadol at 50 mg/kg (2.7 times the MRHD of tramadol on a mg/m2 basis) to pregnant female rats from Gestation Days 10 to 21 caused structural abnormalities in the brains of the offspring.
Celecoxib:
Celecoxib at oral doses ≥150 mg/kg/day (approximately 4 times the level of celecoxib of 224 mg at the MRHD of SEGLENTIS based on AUC), caused an increased incidence of ventricular septal defects, a rare event, and fetal alterations, such as ribs fused, sternebrae fused and sternebrae misshapen when rabbits were treated throughout organogenesis. A dose-dependent increase in diaphragmatic hernias was observed when rats were given celecoxib at oral doses ≥30 mg/kg/day (approximately 13 times the MRHD based on AUC) throughout organogenesis. In rats, exposure to celecoxib during early embryonic development resulted in pre-implantation and post-implantation losses at oral doses ≥50 mg/kg/day (approximately 13 times the MRHD based on AUC).
Celecoxib produced no evidence of delayed labor or parturition at oral doses up to 100 mg/kg in rats (approximately 15 times the MRHD based on AUC). The effects of SEGLENTIS on labor and delivery in pregnant women are unknown.
8.2 Lactation
Risk Summary
SEGLENTIS is not recommended for obstetrical preoperative medication or for post-delivery analgesia in lactating women because the safety of tramadol in infants and newborns has not been studied.
Tramadol
Tramadol and its metabolite, O-desmethyltramadol (M1), are present in human milk. There is no information on the effects of the drug on the breastfed infant or the effects of the drug on milk production. The M1 metabolite is more potent than tramadol in mu opioid receptor binding [see Clinical Pharmacology (12.1)]. Published studies have reported tramadol and M1 in colostrum with administration of tramadol to breastfeeding mothers in the early post-partum period. Women who are ultra-rapid metabolizers of tramadol may have higher than expected serum levels of M1, potentially leading to higher levels of M1 in breast milk that can be dangerous in their breastfed infants. In women with normal tramadol metabolism, the amount of tramadol secreted into human milk is low and dose dependent. Because of the potential for serious adverse reactions, including excess sedation and respiratory depression in a breastfed infant, advise patients that breastfeeding is not recommended during treatment with SEGLENTIS (see Data) [see Warnings and Precautions (5.8)].
Celecoxib
Limited data from 3 published reports that included a total of 12 breastfeeding women showed low levels of celecoxib in breast milk. The calculated average daily infant dose was 10 to 40 mcg/kg/day, less than 1% of the weight-based therapeutic dose for a two-year old-child. A report of two breastfed infants 17 and 22 months of age did not show any adverse events.
Clinical Considerations
If infants are exposed to SEGLENTIS through breast milk, they should be monitored for excess sedation and respiratory depression. Withdrawal symptoms can occur in breastfed infants when maternal administration of an opioid analgesic is stopped, or when breastfeeding is stopped.
Data
Tramadol
Following a single IV 100 mg dose of tramadol, the cumulative excretion in breast milk within 16 hours post dose was 100 mcg of tramadol (0.1% of the maternal dose) and 27 mcg of M1.
8.3 Females and Males of Reproductive Potential
Infertility
Tramadol
Use of opioids for an extended period of time may cause reduced fertility in females and males of reproductive potential. It is not known whether these effects on fertility are reversible [see Adverse Reactions (6.2), Clinical Pharmacology (12.2)].
Published studies in adult male rodents report that tramadol, at clinically relevant doses, can produce adverse effects on male reproductive hormones and tissues [see Nonclinical Toxicology (13.1)].
Celecoxib
Females:
Based on the mechanism of action, the use of prostaglandin-mediated NSAIDs, including celecoxib, may delay or prevent rupture of ovarian follicles, which has been associated with reversible infertility in some women. Published animal studies have shown that administration of prostaglandin synthesis inhibitors has the potential to disrupt prostaglandin mediated follicular rupture required for ovulation. Small studies in women treated with NSAIDs have also shown a reversible delay in ovulation. Consider withdrawal of NSAIDs, including celecoxib, in women who have difficulties conceiving or who are undergoing investigation of infertility.
8.4 Pediatric Use
The safety and effectiveness of SEGLENTIS in pediatric patients have not been established.
Tramadol
Life-threatening respiratory depression and death have occurred in children who received tramadol [see Warnings and Precautions (5.8)]. In some of the reported cases, these events followed tonsillectomy and/or adenoidectomy, and one of the children had evidence of being an ultra-rapid metabolizer of tramadol (i.e., multiple copies of the gene for cytochrome P450 isoenzyme 2D6). Children with sleep apnea may be particularly sensitive to the respiratory depressant effects of tramadol. Because of the risk of life- threatening respiratory depression and death:
- SEGLENTIS is contraindicated for all children younger than age 12 years of age [see Contraindications (4)].
- SEGLENTIS is contraindicated for post-operative management in pediatric patients younger than 18 years of age following tonsillectomy and/or adenoidectomy [see Contraindications (4)].
Avoid the use of SEGLENTIS in adolescents 12 to 18 years of age who have other risk factors that may increase their sensitivity to the respiratory depressant effects of tramadol unless the benefits outweigh the risks. Risk factors include conditions associated with hypoventilation such as postoperative status, obstructive sleep apnea, obesity, severe pulmonary disease, neuromuscular disease, and concomitant use of other medications that cause respiratory depression.
8.5 Geriatric Use
In the randomized, double-blind, active- and placebo-controlled, parallel group study comparing SEGLENTIS to tramadol, celecoxib, and placebo in patients with acute post-operative pain following unilateral first metatarsal osteotomy with internal fixation, 9.1% of patients were ≥65 years of age. Age subgroup examination was planned by protocol and it revealed a similar trend in efficacy compared to younger patients and no untoward or unexpected adverse reactions were seen in the elderly patients who received SEGLENTIS.
No dose adjustments are required for elderly patients.
Tramadol
Respiratory depression is the chief risk for elderly patients treated with opioids and has occurred after large initial doses were administered to patients who were not opioid-tolerant or when opioids were co-administered with other agents that depress respiration. Frequently reevaluate the patient for signs of central nervous system and respiratory depression [see Warnings and Precautions (5.14)].
Tramadol is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, it may be useful to regularly evaluate renal function.
Celecoxib
Elderly patients, compared to younger patients, are at greater risk for NSAID- associated serious cardiovascular, gastrointestinal, and/or renal adverse reactions. If the anticipated benefit for the elderly patient outweighs these potential risks, monitor patients for adverse effects [see Warnings and Precautions (5.6, 5.7, 5.20, 5.23, 5.31)]. Because SEGLENTIS is approved at a unique dosage of celecoxib, SEGLENTIS is not recommended in patients that require dosages other than 2 tablets every 12 hours, containing a total daily dose of celecoxib of 224 mg.
Of the total number of patients who received celecoxib in pre-approval clinical trials, more than 3,300 were 65-74 years of age, while approximately 1,300 additional patients were 75 years and over. No substantial differences in effectiveness were observed between these subjects and younger subjects. In clinical studies comparing renal function as measured by the GFR, BUN and creatinine, and platelet function as measured by bleeding time and platelet aggregation, the results were not different between elderly and young volunteers.
However, as with other NSAIDs, including those that selectively inhibit COX-2, there have been more spontaneous post-marketing reports of fatal GI events and acute renal failure in the elderly than in younger patients [see Warnings and Precautions (5.7, 5.23)].
8.6 Renal Impairment
Because SEGLENTIS contains celecoxib, the use of SEGLENTIS in patients with severe renal impairment is not recommended [see Warnings and Precautions (5.23) and Clinical Pharmacology (12.3)].
The pharmacokinetics and tolerability of SEGLENTIS in patients with renal impairment has not been studied.
Tramadol
Impaired renal function results in a decreased rate and extent of excretion of tramadol and its active metabolite, M1. With the prolonged half-life in these conditions, achievement of steady state is delayed, so that it may take several days for elevated plasma concentrations to develop.
8.7 Hepatic Impairment
As tramadol and celecoxib are both extensively metabolized by the liver, the use of SEGLENTIS in patients with moderate and severe hepatic impairment is not recommended [see Warnings and Precautions (5.20), Clinical Pharmacology (12.3)].
The pharmacokinetics and tolerability of SEGLENTIS in patients with impaired hepatic function have not been studied.
Tramadol
Metabolism of tramadol and M1 is reduced in patients with severe hepatic impairment based on a study in patients with advanced cirrhosis of the liver.
Celecoxib
The daily recommended dose of celecoxib capsules in patients with moderate hepatic impairment (Child-Pugh Class B) should be reduced by 50%. Because the dose of celecoxib and tramadol cannot be adjusted individually for SEGLENTIS, the use in moderate hepatic impairment is not recommended. The use of celecoxib in patients with severe hepatic impairment is not recommended [see Clinical Pharmacology (12.3)].
8.8 Poor Metabolizers of CYP2C9 Substrates
Celecoxib
In patients who are known or suspected to be poor CYP2C9 metabolizers (i.e., CYP2C9*3/*3), based on genotype or previous history/experience with other CYP2C9 substrates (such as warfarin, phenytoin) celecoxib is administered starting with half the lowest recommended dose [see Clinical Pharmacology (12.5)]. Because SEGLENTIS is not available in lower strengths of celecoxib, SEGLENTIS is not recommended in patients who are known or suspected to be poor CYP2C9 metabolizers [see Clinical Pharmacology (12.5)].
Pregnancy: May cause fetal harm (8.1)
Lactation: Breastfeeding not recommended (8.2).
Severe Renal Impairment: Use not recommended (8.6).
Moderate and Severe Hepatic Impairment: Use not recommended (8.7).
Poor Metabolizers of CYP2C9: Due to the inability to start SEGLENTIS at a lower dose, use of SEGLENTIS is not recommended (8.8).
CLINICAL PHARMACOLOGY SECTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
SEGLENTIS is a co-crystal that contains tramadol, an opioid agonist and inhibitor of norepinephrine and serotonin re-uptake, and celecoxib, a nonsteroidal anti-inflammatory drug, in a 1:1 molecular ratio.
Tramadol
Although the mode of action of tramadol is not completely understood, the analgesic effect of tramadol is believed to be due to both binding to µ-opioid receptors and weak inhibition of reuptake of norepinephrine and serotonin.
Opioid activity of tramadol is due to both low affinity binding of the parent compound and higher affinity binding of the O-demethylated metabolite M1 to µ-opioid receptors. In animal models, M1 is up to 6 times more potent than tramadol in producing analgesia and 200 times more potent in µ-opioid binding. Tramadol-induced analgesia is only partially antagonized by the opiate antagonist naloxone in several animal tests. The relative contribution of both tramadol and M1 to human analgesia is dependent upon the plasma concentrations of each compound [see Clinical Pharmacology (12.2)].
Celecoxib
Celecoxib is an analgesic, anti-inflammatory, and antipyretic properties. The mechanism of action of celecoxib is believed to be due to inhibition of prostaglandin synthesis, primarily via inhibition of cyclooxygenase-2 (COX-2).
Celecoxib is a potent inhibitor of prostaglandin synthesis in vitro. Celecoxib concentrations reached during therapy have produced in vivo effects. Prostaglandins sensitize afferent nerves and potentiate the action of bradykinin in inducing pain in animal models. Prostaglandins are mediators of inflammation. Since celecoxib is an inhibitor of prostaglandin synthesis, its mode of action may be due to a decrease of prostaglandins in peripheral tissues.
12.2 Pharmacodynamics
Effects on the Central Nervous System
Tramadol produces respiratory depression by direct action on brain stem respiratory centers. The respiratory depression involves a reduction in the responsiveness of the brain stem respiratory centers to both increases in carbon dioxide tension and electrical stimulation.
Tramadol administration may produce a constellation of symptoms including nausea and vomiting, dizziness, and somnolence.
Tramadol causes miosis, even in total darkness. Pinpoint pupils are a sign of opioid overdose but are not pathognomonic (e.g., pontine lesions of hemorrhagic or ischemic origins may produce similar findings). Marked mydriasis rather than miosis may be seen due to hypoxia in overdose situations.
Effects on the Gastrointestinal Tract and Other Smooth Muscle
Tramadol causes a reduction in motility associated with an increase in smooth muscle tone in the antrum of the stomach and duodenum. Digestion of food in the small intestine is delayed and propulsive contractions are decreased. Propulsive peristaltic waves in the colon are decreased, while tone may be increased to the point of spasm resulting in constipation. Other opioid- induced effects may include a reduction in biliary and pancreatic secretions, spasm of sphincter of Oddi, and transient elevations in serum amylase.
Effects on the Cardiovascular System
Tramadol produces peripheral vasodilation which may result in orthostatic hypotension or syncope. Manifestations of histamine release and/or peripheral vasodilation may include pruritus, flushing, red eyes, sweating, and/or orthostatic hypotension.
The effect of oral tramadol on the QTcF interval was evaluated in a double- blind, randomized, four-way crossover, placebo-and positive-(moxifloxacin) controlled study in 68 adult male and female healthy subjects. At a 600 mg/day dose (1.5-fold the maximum immediate-release daily dose), the study demonstrated no significant effect on the QTcF interval.
Effects on the Endocrine System
Opioids inhibit the secretion of adrenocorticotropic hormone (ACTH), cortisol, and luteinizing hormone (LH) in humans [see Warnings and Precautions (5.15), Adverse Reactions (6.2)]. They also stimulate prolactin, growth hormone (GH) secretion, and pancreatic secretion of insulin and glucagon.
Use of opioids for an extended period of time may influence the hypothalamic- pituitary-gonadal axis, leading to androgen deficiency that may manifest as low libido, impotence, erectile dysfunction, amenorrhea, or infertility. The causal role of opioids in the clinical syndrome of hypogonadism is unknown because the various medical, physical, lifestyle, and psychological stressors that may influence gonadal hormone levels have not been adequately controlled for in studies conducted to date [see Adverse Reactions (6.2)].
Effects on the Immune System
Opioids have been shown to have a variety of effects on components of the immune system in in vitro and animal models. The clinical significance of these findings is unknown. Overall, the effects of opioids appear to be modestly immunosuppressive.
Concentration–Efficacy Relationships
The minimum effective analgesic concentration will vary widely among patients, especially among patients who have been previously treated with opioid agonists. The minimum effective analgesic concentration of tramadol for any individual patient may increase over time due to an increase in pain, the development of a new pain syndrome and/or the development of analgesic tolerance [see Dosage and Administration (2)].
Concentration–Adverse Reaction Relationships
There is a relationship between increasing tramadol plasma concentration and increasing frequency of dose-related opioid adverse reactions such as nausea, vomiting, CNS effects, and respiratory depression. In opioid-tolerant patients, the situation may be altered by the development of tolerance to opioid-related adverse reactions [see Dosage and Administration (2)].
Platelets
In clinical trials using normal volunteers, celecoxib at single doses up to 800 mg and multiple doses of 600 mg twice daily for up to 7 days duration (higher than recommended therapeutic doses) had no effect on reduction of platelet aggregation or increase in bleeding time. Because of its lack of platelet effects, celecoxib is not a substitute for aspirin for cardiovascular prophylaxis. It is not known if there are any effects of celecoxib on platelets that may contribute to the increased risk of serious cardiovascular thrombotic adverse events associated with the use of celecoxib.
Fluid Retention
Inhibition of PGE2 synthesis may lead to sodium and water retention through increased reabsorption in the renal medullary thick ascending loop of Henle and perhaps other segments of the distal nephron. In the collecting ducts, PGE2 appears to inhibit water reabsorption by counteracting the action of antidiuretic hormone.
12.3 Pharmacokinetics
Absorption
Tramadol is presented in SEGLENTIS as a racemate. After Tramadol immediate- release (IR) administration both the [-] and [+] forms of both tramadol and M1 are detected in the circulation.
The rate and extent of absorption of tramadol and celecoxib in SEGLENTIS show differences in absorption compared to Tramadol IR Tablets or Celecoxib capsule when those drugs are administered individually and concomitantly in a single four way cross-over study.
The PK parameters of tramadol, tramadol-M1 metabolite and celecoxib after single dose oral administration of SEGLENTIS Tablets, Tramadol IR Tablets, Celecoxib Capsule or Tramadol IR Tablets and Celecoxib Capsule administered concomitantly is shown in Table 3.
Table 3: The PK parameters of tramadol, tramadol-M1 metabolite and celecoxib after single dose oral administration of SEGLENTIS Tablets, Tramadol IR Tablets, Celecoxib Capsule, or Tramadol IR Tablets and Celecoxib Capsule administered concomitantly in four way cross-over study (male and female participants receiving all treatments in random order).|
Analyte |
PK Parameter * |
2 × SEGLENTIS Tablets (112 mg celecoxib + 88 mg tramadol) |
2 × 50 mg Tramadol IR Tablets |
1× 100 mg Celecoxib Capsule |
2 × 50 mg Tramadol IR Tablets + 100 mg Celecoxib Capsule |
|---|---|---|---|---|---|
|
n=33 |
n=32 |
n=33 |
n=32 | ||
Þ | |||||
|
Tramadol |
Cmax (ng/mL) |
214 (29) |
305 (23) |
|
312 (22) |
|
Tmax (h) † |
3.0 (1.25, 8.0) |
2.0 (0.75, 3.0) |
|
1.9 (1.0, 6.0) | |
|
AUC0-t (ng∙h/mL) |
2507 (36) |
2709 (35) |
|
2888 (34) | |
|
AUC0-∞ (ng∙h/mL) |
2590 (35) ‡ |
2802(32) § |
|
2990 (32) § | |
|
T½ (h) |
6.5 (15) |
6.1 (17) |
|
6.2 (16) | |
|
Tramadol-M1 metabolite |
Cmax (ng/mL) |
55 (29) |
78 (29) |
|
78 (29) |
|
Tmax (h) † |
4.0 (2.5, 8.0) |
2.5 (1.25, 6.0) |
|
2.5 (1.25, 8.0) | |
|
AUC0-t (ng∙h/mL) |
846 (27) |
965 (25) |
|
1010 (25) | |
|
AUC0-∞ (ng∙h/mL) |
880 (24) ‡ |
1002 (21) § |
|
1049 (21) § | |
|
T½ (h) |
7.2 (14) |
6.7 (14) |
|
7.0 (15) | |
|
Celecoxib |
Cmax (ng/mL) |
259 (34) |
|
318 (47) |
165 (46) |
|
Tmax (h) † |
1.5 (0.75, 6.0) |
|
3.0 (1.25, 8.0) |
2.5 (1.0, 12.0) | |
|
AUC0-t (ng∙h/mL) |
1930 (41) |
|
2348 (40) |
1929 (38) | |
|
AUC0-∞ (ng∙h/mL) |
2128 (42) ¶ |
|
2553 (43) # |
2224 (39) Þ | |
|
T½ (h) |
13 (27) |
|
11 (46) |
14 (29) |
Multiple dose
After multiple dose administration of SEGLENTIS tablets twice daily for a total of 15 consecutive doses, the steady-state accumulation ratio of tramadol Cmax and AUCτ (15th dose/ 1st dose) were 2.20-fold and 2.37-fold, respectively. The steady-state accumulation ratio of celecoxib Cmax and AUCτ (15th dose/ 1st dose) were 1.76-fold and 2.15-fold, respectively. Based on pre-dose concentrations, the steady state appears to be achieved for all three analytes, tramadol, M1 metabolite and celecoxib, of SEGLENTIS tablets.
The absolute oral bioavailability of tramadol and celecoxib from SEGLENTIS have not been determined. Tramadol has a mean absolute bioavailability of approximately 75% following administration of a single 100 mg oral dose of tramadol tablets. Absolute bioavailability studies have not been conducted for celecoxib.
Tramadol:
In general, both enantiomers of tramadol and M1 follow a parallel time course in the body following single and multiple doses although small differences (~ 10%) exist in the absolute amount of enantiomer present. Steady-state plasma concentrations of both tramadol and M1 are achieved within two days with four times per day dosing. There is no evidence of self-induction.
Celecoxib:
The coadministration of celecoxib with an aluminum- and magnesium-containing antacids resulted in a reduction in plasma celecoxib concentrations with a decrease of 37% in Cmax and 10% in AUC.
Food Effect
When SEGLENTIS tablets were administered with a high-fat, high-calorie meal, the Cmax and the AUC of tramadol and tramadol-M1 metabolite were not significantly affected. For celecoxib, component of SEGLENTIS tablets, the Tmax was delayed by approximately 2.5 hour and resulted in around a 30% increase in Cmax and AUC, which was approximately similar to the food effect of Celecoxib capsule. SEGLENTIS can be administered without regard to timing of meals.
Distribution
Tramadol
The volume of distribution of tramadol was 2.6 and 2.9 L/kg in male and female subjects, respectively, following a 100 mg intravenous dose. The binding of tramadol to human plasma proteins is approximately 20% and binding also appears to be independent of concentration up to 10 mcg/mL. Saturation of plasma protein binding occurs only at concentrations outside the clinically relevant range.
Celecoxib
In healthy subjects, celecoxib is highly protein bound (~ 97%) within the clinical dose range. In vitro studies indicate that celecoxib binds primary to albumin and, to a lesser extent, α1-acid glycoprotein. The apparent volume of distribution at steady state (Vss/F) is approximately 400 L suggesting extensive distribution into the tissues. Celecoxib is not preferentially bound to red blood cells.
Elimination
Tramadol is eliminated primarily through metabolism by the liver and the metabolites are eliminated primarily by the kidneys.
The mean terminal plasma elimination half-life of tramadol were 6.5 hours and 9.0 hours after single-dose and multiple-dose administration of SEGLENTIS tablets, respectively. There was no change in the elimination half-life of celecoxib (13 hours) after single or multiple dose administration of SEGLENTIS tablets.
Metabolism
Tramadol:
Tramadol is extensively metabolized by a number of pathways, including CYP2D6 and CYP3A4, as well as by conjugation of parent and metabolites.
Approximately 30% of the dose is excreted in the urine as unchanged drug, whereas 60% of the dose is excreted as metabolites. The remainder is excreted either as unidentified or as unextractable metabolites.
The major metabolic pathways appear to be N- and O-demethylation and glucuronidation or sulfation in the liver. One metabolite (O-desmethyltramadol, denotated M1) is pharmacologically active in animal models. Formation of M1 is dependent on CYP2D6 and as such is subject to inhibition, which may affect the therapeutic response [see Warnings and Precautions (5.8); Drug Interactions (7)].
Approximately 7% of the population has reduced activity of the CYP2D6 isoenzyme of cytochrome P450. These individuals are "poor metabolizers" of debrisoquine, dextromethorphan, and tricyclic antidepressants, among other drugs. Based on a population PK analysis of Phase 1 studies in healthy subjects, concentrations of tramadol were approximately 20% higher in "poor metabolizers" versus "extensive metabolizers," while M1 concentrations were 40% lower. Concomitant therapy with inhibitors of CYP2D6 such as fluoxetine, paroxetine and quinidine could result in significant drug interactions.
In vitro drug interaction studies in human liver microsomes indicate that inhibitors of CYP2D6 such as fluoxetine and its metabolite norfluoxetine, amitriptyline and quinidine inhibit the metabolism of tramadol to various degrees, suggesting that concomitant administration of these compounds could result in increases in tramadol concentrations and decreased concentrations of M1. The full pharmacological impact of these alterations in terms of either efficacy or safety is unknown. Concomitant use of serotonin re-uptake inhibitors and MAO inhibitors may enhance the risk of adverse events, including seizure and serotonin syndrome [see Warnings and Precautions (5.11, 5.12) and Drug Interactions (7)].
Celecoxib:
Celecoxib metabolism is primarily mediated via CYP2C9. Three metabolites, a primary alcohol, the corresponding carboxylic acid, and its glucuronide conjugate, have been identified in human plasma. These metabolites are inactive as COX-1 or COX-2 inhibitors.
Excretion
Tramadol:
Approximately 30% of the dose is excreted in the urine as unchanged drug, whereas 60% of the dose is excreted as metabolites.
Celecoxib:
Celecoxib is eliminated predominantly by hepatic metabolism with little (<3%) unchanged drug recovered in the urine and feces. Following a single oral dose of radiolabeled drug, approximately 57% of the dose was excreted in the feces and 27% was excreted into the urine. The primary metabolite in both urine and feces was the carboxylic acid metabolite (73% of dose) with low amounts of the glucuronide also appearing in the urine. It appears that the low solubility of the drug prolongs the absorption process making terminal half-life (T1/2) determinations more variable. The effective half-life is approximately 11 hours under fasted conditions. The apparent plasma clearance (CL/F) is about 500 mL/min.
Specific Populations
Geriatric Patients
Tramadol:
Healthy elderly subjects aged 65 to 75 years have plasma tramadol concentrations and elimination half-lives comparable to those observed in healthy subjects less than 65 years of age. In subjects over 75 years, maximum serum concentrations are elevated (208 vs. 162 ng/mL) and the elimination half-life is prolonged (7 vs. 6 hours) compared to subjects 65 to 75 years of age [see Use in Specific Populations (8.5)].
Celecoxib:
At steady state, elderly subjects (over 65 years old) had a 40% higher Cmax and a 50% higher AUC compared to the young subjects. In elderly females, celecoxib Cmax and AUC are higher than those for elderly males, but these increases are predominantly due to lower body weight in elderly females.
Pediatric Patients
Pharmacokinetics of SEGLENTIS has not been established in pediatric patients.
Sex
Sex effects on the Pharmacokinetics of SEGLENTIS have not been assessed.
The absolute bioavailability of tramadol was 73% in males and 79% in females. The plasma clearance was 6.4 mL/min/kg in males and 5.7 mL/min/kg in females following a 100 mg IV dose of tramadol. Following a single oral dose, and after adjusting for body weight, females had a 12% higher peak tramadol concentration and a 35% higher area under the concentration-time curve compared to males. The clinical significance of this difference is unknown.
Race
Race effects on the Pharmacokinetics of SEGLENTIS have not been assessed.
Celecoxib:
Meta-analysis of pharmacokinetic studies has suggested an approximately 40% higher AUC of celecoxib in Blacks compared to Caucasians. The cause and clinical significance of this finding is unknown.
Renal Impairment
Impaired renal function results in a decreased rate and extent of excretion of tramadol and its active metabolite, M1.
In a cross-study comparison, celecoxib AUC was approximately 40% lower in patients with chronic renal insufficiency (GFR 35-60 mL/min) than that seen in subjects with normal renal function. No significant relationship was found between GFR and celecoxib clearance. Patients with severe renal insufficiency have not been studied [see Use in Specific Populations (8.6), Warnings and Precautions (5.23)].
Hepatic Impairment
Metabolism of tramadol and M1 is reduced in patients with severe hepatic impairment based on a study in patients with advanced cirrhosis of the liver, resulting in both a larger area under the concentration time curve for tramadol and longer tramadol and M1 elimination half-lives (13 hrs. for tramadol and 19 hrs. for M1).
A pharmacokinetic study in subjects with mild (Child-Pugh Class A) and moderate (Child-Pugh Class B) hepatic impairment has shown that steady state celecoxib AUC is increased about 40% and 180%, respectively, above that seen in healthy control subjects [see Use in Specific Populations (8.7)].
Drug Interaction Studies
In vitro studies indicate that celecoxib is not an inhibitor of CYP2C9, 2C19 or 3A4.
In vivo studies have shown the following:
Aspirin
When NSAIDs were administered with aspirin, the protein binding of NSAIDs were reduced, although the clearance of free NSAID was not altered. The clinical significance of this interaction is not known. See Table 3 for clinically significant drug interactions of NSAIDs with aspirin [see Drug Interactions (7)].
Lithium
In a study conducted in healthy subjects, mean steady-state lithium plasma levels increased approximately 17% in subjects receiving lithium 450 mg twice daily with celecoxib 200 mg twice daily as compared to subjects receiving lithium alone [see Drug Interactions (7)].
Fluconazole
Concomitant administration of fluconazole at 200 mg once daily resulted in a two-fold increase in celecoxib plasma concentration. This increase is due to the inhibition of celecoxib metabolism via P450 2C9 by fluconazole [see Drug Interactions (7)].
Other Drugs
The effects of celecoxib on the pharmacokinetics and/or pharmacodynamics of glyburide, ketoconazole, [see Drug Interactions (7)], phenytoin, and tolbutamide have been studied in vivo and clinically important interactions have not been found.
Tramadol and Celecoxib
Tramadol is extensively metabolized by a number of pathways, including CYP2D6 and CYP3A4. The formation of tramadol M1 metabolite is dependent on CYP2D6. In vitro studies indicate that celecoxib is an inhibitor of CYP2D6.
An in vivo multiple dose PK study of 100 mg tramadol (2×50 mg) and 100 mg celecoxib (1×100 mg) administered concomitantly twice daily for 15 doses demonstrates that steady-state Cmax and AUC of tramadol and its active metabolite M1 are comparable along with comparable PK profiles to the 100 mg tramadol (2×50 mg) administered alone twice daily for 15 doses. The study results indicate that co-administration of celecoxib does not appear to affect the PK of tramadol or M1.
12.5 Pharmacogenomics
Poor Metabolizers of CYP2C9
CYP2C9 activity is reduced in individuals with genetic polymorphisms that lead to reduced enzyme activity, such as those homozygous for the CYP2C92 and CYP2C93 polymorphisms. Limited data from 4 published reports that included a total of 8 subjects with the homozygous CYP2C9*3/3 genotype showed celecoxib systemic levels that were 3- to 7-fold higher in these subjects compared to subjects with CYP2C91/*1 or *I/*3 genotypes. The pharmacokinetics of celecoxib have not been evaluated in subjects with other CYP2C9 polymorphisms, such as *2, *5, *6, *9 and *11. It is estimated that the frequency of the homozygous *3/*3 genotype is 0.3% to 1.0% in various ethnic groups [see Use in Specific Populations (8.8)].
Poor / Extensive Metabolizers of CYP2D6
The formation of the active metabolite, M1, is mediated by CYP2D6. Approximately 7% of the population has reduced activity of the CYP2D6. These individuals are "poor metabolizers" of debrisoquine, dextromethorphan, and tricyclic antidepressants, among other drugs. Based on a population PK analysis of Phase I studies with immediate-release tablets in healthy subjects, concentrations of tramadol were approximately 20% higher in "poor metabolizers" versus "extensive metabolizers," while M1 concentrations were 40% lower.
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
There are no animal or laboratory studies with SEGLENTIS (product composed of tramadol and celecoxib) to evaluate carcinogenesis, mutagenesis, or impairment of fertility. Data on the individual components are described below.
Carcinogenesis
Tramadol
A slight but statistically significant increase in two common murine tumors, pulmonary and hepatic, was observed in an NMRI mouse carcinogenicity study, particularly in aged mice. Mice were dosed orally up to 30 mg/kg in the drinking water (0.8 times the maximum recommended human dose (MRHD) of tramadol at 176 mg on a mg/m2 basis) for approximately two years, although the study was not done with the Maximum Tolerated Dose. This finding is not believed to suggest risk in humans. No evidence of carcinogenicity was noted in a rat 2-year carcinogenicity study testing oral doses of up to 30 mg/kg in the drinking water (1.7 times the MRHD of tramadol on a mg/m2 basis).
Celecoxib
Celecoxib was not carcinogenic in Sprague-Dawley rats given oral doses up to 200 mg/kg for males and 10 mg/kg for females (approximately 4 to 9 times the MRHD based on AUC) or in mice given oral doses up to 25 mg/kg for males and 50 mg/kg for females (approximately 2.2 times the MRHD based on AUC) for two years.
Mutagenesis
Tramadol
Tramadol was mutagenic in the presence of metabolic activation in the mouse lymphoma assay. Tramadol was not mutagenic in the in vitro bacterial reverse mutation assay using Salmonella and E. coli (Ames), the mouse lymphoma assay in the absence of metabolic activation, the in vitro chromosomal aberration assay, or the in vivo micronucleus assay in bone marrow.
Celecoxib
Celecoxib was not mutagenic in an Ames test and a mutation assay in Chinese hamster ovary (CHO) cells, nor clastogenic in a chromosome aberration assay in CHO cells and an in vivo micronucleus test in rat bone marrow.
Impairment of Fertility
Tramadol
No effects on fertility were observed for tramadol at oral dose levels up to 50 mg/kg in male rats and 75 mg/kg in female rats. These dosages are 2.7 and 4.1 times the maximum recommended human dose (MRHD) of tramadol (176 mg) on a mg/m2 basis, respectively [see Use in Specific Populations (8.3)].
However, published studies report that treatment of adult male rats with tramadol (40 mg/kg, IP and SC for 30 and 60 days, respectively, 2.2 times the MRHD of tramadol on a mg/m2 basis; or 4.5 to 135 mg/kg, SC for 18 weeks, 0.2 to 7.4 times the MRHD of tramadol on a mg/m2 basis) produced adverse effects on male reproductive hormones and male reproductive tissues.
Celecoxib
Celecoxib had no effect on male or female fertility or male reproductive function in rats at oral doses up to 600 mg/kg/day (approximately 24 times the MRHD of celecoxib (224 mg) based on AUC). At ≥50 mg/kg/day (approximately 13 times the MRHD of celecoxib (224 mg) based on AUC) there was increased preimplantation loss.
13.2 Animal Toxicology and/or Pharmacology
Celecoxib
An increase in the incidence of background findings of spermatocele with or without secondary changes such as epididymal hypospermia as well as minimal to slight dilation of the seminiferous tubules was seen in the juvenile rat. These reproductive findings while apparently treatment related did not increase in incidence or severity with dose and may indicate an exacerbation of a spontaneous condition. Similar reproductive findings were not observed in studies of juvenile or adult dogs or in adult rats treated with celecoxib. The clinical significance of this observation is unknown.
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
SEGLENTIS study on acute pain after bunionectomy with osteotomy
The efficacy and safety of SEGLENTIS was evaluated in one randomized, double- blind, parallel group study comparing SEGLENTIS to tramadol, celecoxib, and placebo (NCT03108482). The study enrolled 637 patients 18 years of age or older (age ranged between 18 and 77) with acute post-operative pain (≥5 and ≤9 on a 0-10 Numeric Pain Rating Scale [NPRS]) following unilateral first metatarsal osteotomy with internal fixation. Patients were randomized at a ratio of 2:2:2:1 to SEGLENTIS 200 mg every 12 hours, tramadol 50 mg every 6 hours, celecoxib 100 mg every 12 hours, or placebo in a double-blind, double- dummy study. Use of rescue medication (acetaminophen and oxycodone HCl) was permitted during the study. Patients had a mean baseline pain intensity of 6.7 on the NPRS.
The primary efficacy endpoint was time-weighted summed pain intensity difference over 48 hours (SPID48). Patients in the SEGLENTIS group had statistically significantly better mean SPID48 scores than any of the other groups after bunionectomy. Pain intensity difference from baseline over 48 hours mean values by treatment group are shown in Figure 1.
Figure 1: Pain Intensity Difference by Evaluation Time Point from Baseline to 48 hours – Post Operative Bunionectomy with Osteotomy (Full Analysis Set Population)
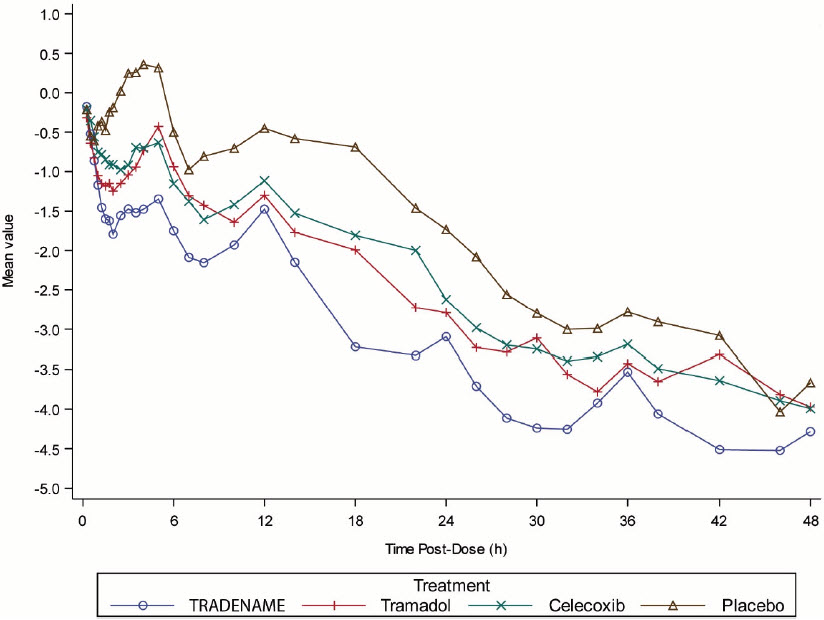
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
SEGLENTIS (celecoxib and tramadol hydrochloride) tablets are coated tablets containing celecoxib 56 mg and tramadol hydrochloride 44 mg. The tablets are white to off-white elongated coated tablets debossed with "100 on one side and "CTC" on the other side and are available as follows:
Bottles of 35 tablets: NDC 66869-564-35
Bottles of 90 tablets: NDC 66869-564-90
Bottles of 90 tablets (Bottle only): NDC 66869-564-09
Dispense in a tight container. Store at 20°C - 25°C (68°F - 77°F); excursions permitted to 15°C - 30°C (59°F - 86°F) [see USP Controlled Room Temperature].