
Amlodipine and Benazepril Hydrochloride
These highlights do not include all the information needed to use AMLODIPINE AND BENAZEPRIL HYDROCHLORIDE CAPSULES safely and effectively. See full prescribing information for AMLODIPINE AND BENAZEPRIL HYDROCHLORIDE CAPSULES. AMLODIPINE AND BENAZEPRIL HYDROCHLORIDE capsules, for oral use Initial U.S. Approval: 1995
97b38387-ae7c-484a-af01-773bd8556b0d
HUMAN PRESCRIPTION DRUG LABEL
Apr 27, 2023
A-S Medication Solutions
DUNS: 830016429
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Amlodipine and Benazepril Hydrochloride
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (14)
Drug Labeling Information
Dosage & Administration Section
2 DOSAGE AND ADMINISTRATION
2.1 General Considerations
The recommended initial dose is amlodipine 2.5 mg and benazepril 10 mg orally once-daily.
Begin therapy with amlodipine and benazepril hydrochloride capsules only after a patient has either (a) failed to achieve the desired antihypertensive effect with amlodipine or benazepril monotherapy, or (b) demonstrated inability to achieve adequate antihypertensive effect with amlodipine therapy without developing edema.
The antihypertensive effect of amlodipine and benazepril hydrochloride capsules is largely attained within 2 weeks. If blood pressure remains uncontrolled, the dose may be titrated up to amlodipine 10 mg and benazepril 40 mg once-daily. The dosing should be individualized and adjusted according to the patient’s clinical response.
In clinical trials of amlodipine and benazepril combination therapy using amlodipine doses of 2.5 to 10 mg and benazepril doses of 10 to 40 mg, the antihypertensive effects increased with increasing dose of amlodipine in all patient groups, and the effects increased with increasing dose of benazepril in nonblack groups.
2.2 Replacement Therapy
Amlodipine and benazepril hydrochloride capsules may be substituted for the titrated components.
- Usual starting dose is 2.5 mg/10 mg. (2.1)
- May be used as add-on therapy for patients not adequately controlled with either a dihydropyridine calcium channel blocker or an ACE inhibitor (2.2)
- Patients who experience edema with amlodipine may be switched to amlodipine and benazepril hydrochloride capsules containing a lower dose of amlodipine. (2.1)
Description Section
11 DESCRIPTION
Amlodipine and benazepril hydrochloride capsules USP are a combination of amlodipine besylate and benazepril hydrochloride.
Benazepril hydrochloride USP is a white to off-white, crystalline powder, soluble (greater than 100 mg/mL) in water, in ethanol, and in methanol. Benazepril hydrochloride’s chemical name is 3-[[1-(ethoxycarbonyl)-3-phenyl-(1S)-propyl]amino]-2,3,4,5-tetrahydro-2-oxo-1H-1-(3S)-benzazepine-1-acetic acid monohydrochloride; its structural formula is:

Its molecular formula is C24H28N2O5•HCl, and its molecular weight is 460.96.
Benazeprilat, the active metabolite of benazepril, is a nonsulfhydryl ACE inhibitor. Benazepril is converted to benazeprilat by hepatic cleavage of the ester group.
Amlodipine besylate USP is a white or almost white powder, slightly soluble in water and sparingly soluble in ethanol. Its chemical name is (R,S)3-ethyl-5-methyl-2-(2-aminoethoxymethyl)-4-(2-chlorophenyl)-1,4-dihydro-6-methyl-3,5-pyridinedicarboxylate benzenesulfonate; its structural formula is:
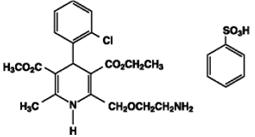
Its molecular formula is C20H25ClN2O5•C6H6O3S, and its molecular weight is 567.1.
Amlodipine besylate is the besylate salt of amlodipine, a dihydropyridine calcium channel blocker.
Amlodipine and benazepril hydrochloride is available as capsules containing amlodipine besylate USP (3.5 mg, 6.9 mg or 13.9 mg, equivalent to 2.5 mg, 5 mg or 10 mg of amlodipine respectively), with 10 mg, 20 mg, or 40 mg of benazepril hydrochloride USP providing for the following available combinations: 2.5 mg/10 mg, 5 mg/10 mg, 5 mg/20 mg, 5 mg/40 mg, 10 mg/20 mg, and 10 mg/40 mg.
The inactive ingredients of the capsules are colloidal silicon dioxide, crospovidone, gelatin, magnesium stearate, microcrystalline cellulose, povidone, sodium lauryl sulfate, and titanium dioxide. In addition, the hard gelatin capsule shells of 5 mg/10 mg contains iron oxide black, iron oxide red, and iron oxide yellow, 5 mg/20 mg contains iron oxide red, 5 mg/40 mg and 10 mg/40 mg contains FD&C Blue 1, FD&C Red 3, and 10 mg/20 mg contains D&C Red 28, FD&C Blue 1, FD&C Red 40, and FD&C Yellow 5. The capsules are printed with edible ink containing black iron oxide and shellac.
Nonclinical Toxicology Section
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity and mutagenicity studies have not been conducted with this combination. However, these studies have been conducted with amlodipine and benazepril alone (see below). No adverse effects on fertility occurred when the benazepril:amlodipine combination was given orally to rats of either sex at doses up to 15:7.5 mg (benazepril:amlodipine)/kg/day, prior to mating and throughout gestation.
Benazepril:****No evidence of carcinogenicity was found when benazepril was administered to rats and mice for up to 2 years at doses of up to 150 mg/kg/day. When compared on the basis of body surface area, this dose is 18 and 9 times (rats and mice, respectively) the maximum recommended human dose (MRHD) (calculations assume a patient weight of 60 kg). No mutagenic activity was detected in the Ames test in bacteria, in an in vitro test for forward mutations in cultured mammalian cells, or in a nucleus anomaly test. At doses of 50 to 500 mg/kg/day (6 to 60 times the MRHD on a body surface area basis), benazepril had no adverse effect on the reproductive performance of male and female rats.
Amlodipine:****Rats and mice treated with amlodipine maleate in the diet for up to 2 years, at concentrations calculated to provide daily dosage levels of 0.5, 1.25, and 2.5 mg amlodipine/kg/day, showed no evidence of a carcinogenic effect of the drug. For the mouse, the highest dose was, on a body surface area basis, similar to the MRHD of 10 mg amlodipine/day. For the rat, the highest dose was, on a body surface area basis, about two and a half times the MRHD (Calculations based on a 60 kg patient). Mutagenicity studies conducted with amlodipine maleate revealed no drug-related effects at either the gene or chromosome level. There was no effect on the fertility of rats treated orally with amlodipine maleate (males for 64 days and females for 14 days prior to mating) at doses of up to 10 mg amlodipine/kg/day (about 10 times the MRHD of 10 mg/day on a body surface area basis).