
Cisatracurium besylate
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use CISATRACURIUM BESYLATE INJECTION safely and effectively. See full prescribing information for CISATRACURIUM BESYLATE INJECTION. CISATRACURIUM BESYLATE injection, for intravenous use Initial U.S. Approval: 1995
e2719e22-2217-2d0c-e053-2a95a90a5b94
HUMAN PRESCRIPTION DRUG LABEL
Aug 9, 2023
PIRAMAL CRITICAL CARE INC
DUNS: 805600439
Products 2
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Cisatracurium besylate
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (2)
Cisatracurium besylate
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (2)
Drug Labeling Information
ADVERSE REACTIONS SECTION
6 ADVERSE REACTIONS
6.1 Clinical Studies Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice.
Adverse Reactions in Clinical Trials of Cisatracurium Besylate Injection in Surgical Patients
The data presented below are based on studies involving 945 surgical patients who received cisatracurium besylate injection in conjunction with other drugs in US and European clinical studies in a variety of procedures [see Clinical Studies ( 14.1)] .
Table 3 displays adverse reactions that occurred at a rate of less than 1%.
Table 3. Adverse Reactions in Clinical Trials of Cisatracurium Besylate Injection in Surgical Patients
|
Adverse Reaction |
Incidence |
|
Bradycardia |
0.4% |
|
Hypotension |
0.2% |
|
Flushing |
0.2% |
|
Bronchospasm |
0.2% |
|
Rash |
0.1% |
Adverse Reactions in Clinical Trials of Cisatracurium Besylate Injection in Intensive Care UnitPatients
The adverse reactions presented below were from studies involving 68 adult ICU patients who received cisatracurium besylate injection in conjunction with other drugs in US and European clinical studies [see Clinical Studies ( 14.3)] . One patient experienced bronchospasm. In one of the two ICU studies, a randomized and double-blind study of ICU patients using TOF neuromuscular monitoring, there were two reports of prolonged recovery (range: 167 and 270 minutes) among 28 patients administered cisatracurium besylate injection and 13 reports of prolonged recovery (range: 90 minutes to 33 hours) among 30 patients administered vecuronium.
6.2 Postmarketing Experience
The following events have been identified during post-approval use of cisatracurium besylate injection in conjunction with one or more anesthetic agents in clinical practice. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made.
These events have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal connection to cisatracurium besylate injection: anaphylaxis, histamine release, prolonged neuromuscular block, muscle weakness, myopathy.
The most common adverse reactions (0.1% to 0.4%) were bradycardia, hypotension, flushing, bronchospasm, and rash. ( 6.1)
**To report SUSPECTED ADVERSE REACTIONS, contact Piramal Critical Care, Inc. at 1-1-800-414-1901 or FDA at 1-800-FDA-1088 or **www.fda.gov/medwatch.
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
7.1 Clinically Significant Drug Interactions
Table 4 displays clinically significant drug interactions with cisatracurium besylate injection.
Table 4. Clinically Significant Drug Interactions with Cisatracurium Besylate Injection
|
Drug or Drug Class |
Clinical Implications* |
|
Succinylcholine |
The use of succinylcholine prior to cisatracurium besylate injection administration may decrease the time to onset of maximum neuromuscular blockade but has no effect on the duration of neuromuscular blockade. |
|
Inhalational Anesthetics |
Administration of inhalational anesthetics with nitrous oxide/oxygen for greater than 30 minutes to achieve 1.25 Minimum Alveolar Concentration (MAC) may prolong the duration of action of initial and maintenance doses of cisatracurium besylate injection. This may potentiate the neuromuscular blockade. |
|
Antibiotics† Local anesthetics Magnesium salts Procainamide Lithium Quinidine |
May prolong the neuromuscular blockade action of cisatracurium besylate injection |
|
Phenytoin, Carbamazepine |
May increase resistance to the neuromuscular blockade action of cisatracurium besylate injection resulting in shorter durations of neuromuscular blockade and infusion rate requirements may be higher. |
† Examples: aminoglycosides, tetracyclines, bacitracin, polymyxins, lincomycin, clindamycin, colistin, sodium colistimethate |
**7.2 Drugs Without Clinically Significant Drug Interactions With
Cisatracurium Besylate Injection**
In clinical studies, propofol had no effect on the duration of action or dosing requirements for cisatracurium besylate injection. Cisatracurium besylate injection is not compatible with propofol for Y-site administration.
• Succinylcholine: May decrease time to onset of maximum neuromuscular blockade ( 7.1)
• Inhalational anesthetics, antibiotics, local anesthetics, magnesiumsalts, procainamide, lithium, quinidine: May potentiate or prolong neuromuscular blockade action of cisatracurium besylate injection. Use peripheral nerve stimulator and monitor clinical signs of neuromuscular blockade. ( 5.8, 7.1)
• Phenytoin and Carbamazepine: May shorten duration of neuromuscular blockade. Use peripheral nerve stimulator and monitor clinical signs of neuromuscular blockade. ( 5.9, 7.1)
OVERDOSAGE SECTION
10 OVERDOSAGE
Overdosage with neuromuscular blocking agents may result in neuromuscular blockade beyond the time needed for surgery and anesthesia. The primary treatment is maintenance of a patent airway and controlled ventilation until recovery of normal neuromuscular function is assured.
Once recovery from neuromuscular block begins, further recovery may be facilitated by administration of a cholinesterase inhibitor (e.g., neostigmine, edrophonium) in conjunction with an appropriate cholinergic inhibitor. Cholinesterase inhibitors should not be administered when complete neuromuscular blockade is evident or suspected because the reversal of paralysis may not be sufficient to maintain a patent airway and support an appropriate level of spontaneous ventilation.
• Neostigmine: Administration of 0.04 to 0.07 mg/kg of neostigmine at approximately 10% recovery from neuromuscular blockade (range: 0 to 15%) produced 95% recovery of the muscle twitch response and a T 4:T 1 ratio ≥ 70% in an average of 9 to 10 minutes. The times from 25% recovery of the muscle twitch response to a T 4:T 1 ratio ≥ 70% following these doses of neostigmine averaged 7 minutes. The mean 25% to 75% recovery index following reversal was 3 to 4 minutes.
• Edrophonium: Administration of 1 mg/kg of edrophonium at approximately 25% recovery from neuromuscular blockade (range: 16% to 30%) produced 95% recovery and a T 4:T 1 ratio ≥ 70% in an average of 3 to 5 minutes.
For providers treating patients treated with cholinesterase inhibitors:
• Use a peripheral nerve stimulator to evaluate recovery and antagonism of neuromuscular blockade
• Evaluate for evidence of adequate clinical recovery (e.g., 5-second head lift and grip strength).
• Support ventilation until adequate spontaneous ventilation has resumed.
The onset of antagonism may be delayed in the presence of debilitation, cachexia, carcinomatosis, and the concomitant use of certain broad spectrum antibiotics, or anesthetic agents and other drugs which enhance neuromuscular block or separately cause respiratory depression [see Drug Interactions ( 7.1)] . Under such circumstances the management is the same as that of prolonged neuromuscular block.
PATIENT COUNSELING INFORMATION
17 PATIENT COUNSELING INFORMATION
Hypersensitivity Reactions Including Anaphylaxis
Advise the caregiver and/or family that severe hypersensitivity reactions have occurred with cisatracurium besylate injection [see Warnings and Precautions ( 5.4)] .
Manufactured for:
Piramal Critical Care, Inc.
Bethlehem, PA 18017, USA
Product of India
Issued: 11/2022
DESCRIPTION SECTION
11 DESCRIPTION
Cisatracurium besylate injection, USP is a nondepolarizing skeletal neuromuscular blocker for intravenous administration. Compared to other neuromuscular blockers, it is intermediate in its onset and duration of action. Cisatracurium besylate injection, USP contains cisatracurium besylate as the active pharmaceutical ingredient.
Cisatracurium besylate is one of 10 isomers of atracurium besylate and constitutes approximately 15% of that mixture. Cisatracurium besylate is [1 R-[1α, 2α (1'R*,2'R*)]]-2,2'-[1,5-pentanediylbis[oxy(3-oxo-3,1-propanediyl)]]bis[1-[(3,4- dimethoxyphenyl)methyl]-1,2,3,4-tetrahydro-6,7-dimethoxy-2-methylisoquinolinium] dibenzenesulfonate. The molecular formula of the cisatracurium parent bis- cation is C 53H 72N 2O 12 and the molecular weight is 929.2. The molecular formula of cisatracurium as the besylate salt is C 65H 82N 2O 18S 2 and the molecular weight is 1243.49. The structural formula of cisatracurium besylate is:
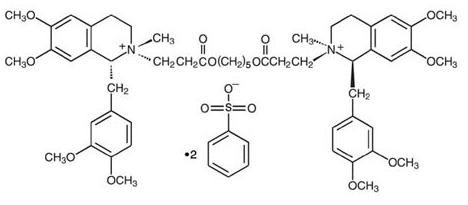
The log of the partition coefficient of cisatracurium besylate is -2.12 in a 1-octanol/distilled water system at 25°C.
Cisatracurium Besylate Injection, USP is a sterile, non-pyrogenic aqueous solution.
Each mL in the single-dose vials contains either 2 mg or 10 mg of cisatracurium (equivalent to 2.68 mg and 13.38 mg of
cisatracurium besylate; respectively), and benzenesulfonic acid as pH adjuster in water for injection.
The pH of cisatracurium besylate Injection is between 3.0 and 3.8.
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
Cisatracurium besylate injection USP is a clear solution supplied as follows:
|
Strength (mg of cisatracurium) |
Containers/Package sizes |
NDC# |
Preservative |
|
10 mg/5 mL (2 mg/mL) |
10 inner cartons. each with one single-dose vial (NDC 66794-245-02), packaged in an outer carton |
66794-245-41 |
Does not contain benzyl alcohol |
|
200 mg/20 mL (10 mg/mL) |
10 inner cartons. each with one single-dose vial (NDC 66794-246-02), packaged in an outer carton |
66794-246-41 |
Does not contain benzyl alcohol |
Discard unused portion of the 5 mL and 20 mL single-dose vials.
Storage
Refrigerate cisatracurium besylate, USP injection at 2° to 8°C (36° to 46°F) in the carton to preserve potency. Protect from light. DO NOT FREEZE. Upon removal of the unused vial from refrigeration to room temperature storage conditions (25°C/77°F), use cisatracurium besylate injection, USP within 21 days, even if re-refrigerated.
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Important Dosage and Administration Instructions
Risk of Medication Errors
Accidental administration of neuromuscular blocking agents may be fatal. Store cisatracurium besylate injection with the cap and ferrule intact and in a manner that minimizes the possibility of selecting the wrong product [see Warnings and Precautions ( 5.5)] .
Important Administration Instructions:
• Cisatracurium besylate injection is for intravenous use only.
• Administer cisatracurium besylate injection in carefully adjusted dosage by or under the supervision of experienced clinicians who are familiar with the drug’s actions and the possible complications.
• Use cisatracurium besylate injection only if the following are immediately available: personnel and facilities for resuscitation and life support (tracheal intubation, artificial ventilation, oxygen therapy); and an antagonist of cisatracurium besylate injection [see Overdosage ( 10)] .
• The dosage information which follows is intended to serve as an initial guide for individual patients; base subsequent cisatracurium besylate injection dosage on the patients’ responses to the initial doses.
• Use a peripheral nerve stimulator to:
○ Determine the adequacy of neuromuscular blockade (e.g., need for additional cisatracurium besylate injection doses, reduction of the infusion rate).
○ Minimize risk of overdosage or underdosage.
○ Assess the extent of recovery from neuromuscular blockade (e.g., spontaneous recovery or recovery after administration of a reversal agent, e.g., neostigmine).
○ Appropriately titrate doses to potentially limit exposure to toxic metabolites.
○ Facilitate more rapid reversal of the cisatracurium besylate injection- induced paralysis.
**2.2 Recommended Cisatracurium Besylate Injection Dose for Performing
Tracheal Intubation**
Tracheal Intubation in Adults
Prior to selecting the initial cisatracurium besylate injection bolus dose, consider the desired time to tracheal intubation and the anticipated length of surgery, factors affecting time to onset of complete neuromuscular block such as age and renal function, and factors that may influence intubation conditions such as the presence of co-induction agents (e.g., fentanyl and midazolam) and the depth of anesthesia.
In conjunction with a propofol/nitrous oxide/oxygen induction-intubation technique or a thiopental/nitrous oxide/oxygen induction-intubation technique, the recommended starting weight-based dose of cisatracurium besylate injection is between 0.15 mg/kg and 0.2 mg/kg administered by bolus intravenous injection. Doses up to 0.4 mg/kg have been safely administered by bolus intravenous injection to healthy patients and patients with serious cardiovascular disease [see Clinical Pharmacology ( 12.2)] .
Patients with Neuromuscular Disease
The maximum recommended initial bolus dose of cisatracurium besylate injection is 0.02 mg/kg in patients with neuromuscular diseases (e.g., myasthenia gravis and myasthenic syndrome and carcinomatosis) [see Warnings and Precautions ( 5.1)] .
Geriatric Patients and Patients with End-Stage Renal Disease
Because the time to maximum neuromuscular blockade is approximately 1 minute slower in geriatric patients compared to younger patients (and in patients with end-stage renal disease than in patients with normal renal function), consider extending the interval between administering cisatracurium besylate injection and attempting intubation by at least 1 minute to achieve adequate intubation conditions in geriatric patients and patients with end-stage renal disease. A peripheral nerve stimulator should be used to determine the adequacy of muscle relaxation for the purposes of intubation and the timing and amounts of subsequent doses [see Use in Specific Populations ( 8.5, 8.6) and Clinical Pharmacology ( 12.3)] .
Tracheal Intubation in Pediatric Patients
Infants 1 to 23 Months of Age
The recommended dose of cisatracurium besylate injection for intubation of pediatric patients ages 1 month to 23 months is 0.15 mg/kg administered over 5 to 10 seconds. When administered during stable opioid/nitrous oxide/oxygen anesthesia, 0.15 mg/kg of cisatracurium besylate injection produced maximum neuromuscular blockade in about 2 minutes (range: 1.3 to 4.3 minutes) with a clinically effective block (time to 25% recovery) for about 43 minutes (range: 34 to 58 minutes) [see Clinical Studies ( 14.2)] .
Pediatric Patients 2 to 12 Years of Age
The recommended weight-based bolus dose of cisatracurium besylate injection for pediatric patients 2 to 12 years of age is 0.1 to 0.15 mg/kg administered over 5 to 10 seconds. When administered during stable opioid/nitrous oxide/oxygen anesthesia, 0.1 mg/kg cisatracurium besylate injection produced maximum neuromuscular blockade in an average of 2.8 minutes (range: 1.8 to 6.7 minutes) with a clinically effective block (time to 25% recovery) for 28 minutes (range: 21 to 38 minutes). When administered during stable opioid/nitrous oxide/oxygen anesthesia, 0.15 mg/kg cisatracurium besylate injection produced maximum neuromuscular blockade in an average of about 3 minutes (range: 1.5 to 8 minutes) with a clinically effective block for 36 minutes (range: 29 to 46 minutes) [see Clinical Studies ( 14.2)] .
**2.3 Recommended Maintenance Bolus Cisatracurium Besylate Injection Doses
in Adult Surgical Procedures**
Determine if maintenance bolus doses are needed based on clinical criteria including the response to peripheral nerve stimulation. The recommended maintenance bolus dose of cisatracurium besylate injection is 0.03 mg/kg; however, smaller or larger maintenance doses may be administered based on the required duration of action. Administer the first maintenance bolus dose starting:
• 40 to 50 minutes after an initial dose of cisatracurium besylate injection 0.15 mg/kg;
• 50 to 60 minutes after an initial dose of cisatracurium besylate injection 0.2 mg/kg.
For long surgical procedures using inhalational anesthetics administered with nitrous oxide/oxygen at the 1.25 MAC level for at least 30 minutes, consider administering less frequent maintenance bolus doses or lower maintenance bolus doses of cisatracurium besylate injection [see Clinical Pharmacology ( 12.2)] . No adjustment to the initial cisatracurium besylate injection maintenance bolus dose should be necessary when cisatracurium besylate injection is administered shortly after initiation of volatile agents or when used in patients receiving propofol anesthesia.
2.4 Dosage in Burn Patients
Burn patients have been shown to develop resistance to nondepolarizing neuromuscular blocking agents; therefore, consider increasing the cisatracurium besylate injection dosages for intubation and maintenance [see Use in Specific Populations ( 8.8)] .
2.5 Dosage for Continuous Infusion
Continuous Infusion for Surgical Procedures in Adults and Pediatric Patients
During extended surgical procedures, cisatracurium besylate injection may be administered by continuous infusion to adults and pediatric patients aged 2 or more years if patients have spontaneous recovery after the initial cisatracurium besylate injection bolus dose. Following recovery from neuromuscular blockade, it may be necessary to re-administer a bolus dose to quickly re-establish neuromuscular blockade prior to starting the continuous infusion.
If patients have had recovery of neuromuscular function, the recommended initial cisatracurium besylate injection infusion rate is 3 mcg/kg/minute [see Dosage and Administration ( 2.6)] . Subsequently reduce the rate to 1 to 2 mcg/kg/minute to maintain continuous neuromuscular blockade. Use peripheral nerve stimulation to assess the level of neuromuscular blockade and to appropriately titrate the cisatracurium besylate injection infusion rate. If no response is elicited to peripheral nerve stimulation, discontinue the infusion until a response returns.
Consider reducing the infusion rate by up to 30% to 40% when cisatracurium besylate injection is administered during stable isoflurane anesthesia for at least 30 minutes (administered with nitrous oxide/oxygen at the 1.25 MAC level) [see Clinical Pharmacology ( 12.2)] . Greater reductions in the cisatracurium besylate injection infusion rate may be required with longer durations of administration of isoflurane or with the administration of other inhalational anesthetics.
Patients Undergoing Coronary Artery Bypass Graft (CABG) Surgery
Consider reducing the infusion rate in patients undergoing CABG with induced hypothermia to half the rate required during normothermia [see Clinical Pharmacology ( 12.2)] . Spontaneous recovery from neuromuscular block following discontinuation of infusion of cisatracurium besylate injection infusion is expected to proceed at a rate comparable to that following administration of a single bolus dose.
Continuous Infusion for Mechanical Ventilation in the Intensive Care Unit in Adults
During extended need for mechanical ventilation and skeletal muscle relaxation in the intensive care unit (ICU), cisatracurium besylate injection may be administered by continuous infusion to adults if a patient has spontaneous recovery of neuromuscular function after the initial cisatracurium besylate injection bolus dose. Following recovery from neuromuscular blockade, it may be necessary to re-administer a bolus dose to quickly re-establish neuromuscular blockade prior to starting the continuous infusion.
The recommended cisatracurium besylate injection infusion rate in adult patients in the ICU is 3 mcg/kg/minute (range: 0.5 to 10.2 mcg/kg/minute) [see Dosage and Administration ( 2.6)] . Use peripheral nerve stimulation to assess the level of neuromuscular blockade and to appropriately titrate the cisatracurium besylate injection infusion rate.
2.6 Rate Tables for Continuous Infusion
The intravenous infusion rate depends upon the cisatracurium besylate injection concentration, the desired dose, the patient's weight, and the contribution of the infusion solution to the fluid requirements of the patient. Tables 1 and 2 provide guidelines for the cisatracurium besylate injection infusion rate, in mL/hour (equivalent to microdrops/minute when 60 microdrops = 1 mL), in concentrations of 0.1 mg/mL or 0.4 mg/mL, respectively.
Table 1. Cisatracurium Besylate Injection Infusion Rates for Maintenance of Neuromuscular Blockade During Opioid/Nitrous Oxide/Oxygen Anesthesia with a Concentration of 0.1 mg/mL
|
Drug Delivery Rate (mcg/kg/minute) | |||||
|
1 |
1.5 |
2 |
3 |
5 | |
|
Patient Weight |
Infusion Delivery Rate (mL/hour) | ||||
|
10 kg |
6 |
9 |
12 |
18 |
30 |
|
45 kg |
27 |
41 |
54 |
81 |
135 |
|
70 kg |
42 |
63 |
84 |
126 |
210 |
|
100 kg |
60 |
90 |
120 |
180 |
300 |
Table 2. Cisatracurium Besylate Injection Infusion Rates for Maintenance of Neuromuscular Blockade During Opioid/Nitrous Oxide/Oxygen Anesthesia with a Concentration of 0.4 mg/mL
|
Drug Delivery Rate (mcg/kg/minute) | |||||
|
1 |
1.5 |
2 |
3 |
5 | |
|
Patient Weight |
Infusion Delivery Rate (mL/hour) | ||||
|
10 kg |
1.5 |
2.3 |
3 |
4.5 |
7.5 |
|
45 kg |
6.8 |
10.1 |
13.5 |
20.3 |
33.8 |
|
70 kg |
10.5 |
15.8 |
21 |
31.5 |
52.5 |
|
100 kg |
15 |
22.5 |
30 |
45 |
75 |
2.7 Preparation of Cisatracurium Besylate Injection
Visually inspect cisatracurium besylate injection for particulate matter and discoloration prior to administration. If a cisatracurium besylate injection solution is cloudy or contains visible particulates, do not use cisatracurium besylate injection. Cisatracurium besylate injection is a colorless to slightly yellow or greenish-yellow solution.
Discard unused portion of the 5 mL and 20 mL single-dose vials.
Cisatracurium besylate injection may be diluted to 0.1 mg/mL in the following solutions:
• 5% Dextrose Injection, USP
• 0.9% Sodium Chloride Injection, USP, or
• 5% Dextrose and 0.9% Sodium Chloride Injection, USP
Store these diluted cisatracurium besylate injection solutions either in a refrigerator or at room temperature for 24 hours without significant loss of potency.
Cisatracurium besylate injection also may be diluted to 0.1 mg/mL or 0.2 mg/mL in the following solution:
• Lactated Ringer’s and 5% Dextrose Injection
Store this diluted cisatracurium besylate injection solution under refrigeration for no more than 24 hours.
Do not dilute cisatracurium besylate injection in Lactated Ringer’s Injection, USP due to chemical instability.
2.8 Drug Compatibility
Cisatracurium besylate injection is compatible and may be administered with the following solutions through Y-site administration:
• 5% Dextrose Injection, USP
• 0.9% Sodium Chloride Injection, USP
• 5% Dextrose and 0.9% Sodium Chloride Injection, USP
• Sufentanil Citrate Injection, diluted as directed
• Alfentanil Hydrochloride Injection, diluted as directed
• Fentanyl Citrate Injection, diluted as directed
• Midazolam Hydrochloride Injection, diluted as directed
• Droperidol Injection, diluted as directed
Cisatracurium besylate injection is acidic (pH = 3.25 to 3.65) and may not be compatible with alkaline solution having a pH greater than 8.5 (e.g., barbiturate solutions). Therefore, do not administer cisatracurium besylate injection and alkaline solutions simultaneously in the same intravenous line.
Cisatracurium besylate injection is not compatible with propofol injection or ketorolac injection for Y-site administration. Compatibility studies with other parenteral products have not been conducted.
Store cisatracurium besylate injection with the cap and ferrule intact and in a manner that minimizes the possibility of selecting the wrong product ( 2.1)
• Administer intravenously only by or under the supervision of experienced clinicians familiar with drug’s actions and possible complications ( 2.1)
• Use only if personnel and facilities for resuscitation and life support, and a cisatracurium besylate injection antagonist are
immediately available ( 2.1)
• Use a peripheral nerve stimulator to determine adequacy of blockade (e.g., need for additional doses), minimize risk of
overdosage or underdosage, assess extent of recovery fromblockade, potentially limit exposure to toxic metabolites through dose titration, and facilitate more rapid reversal of cisatracuriumbesylate injection-induced paralysis ( 2.1)
• See Full Prescribing information for:
○ Dosage and administration instructions in adults, pediatricpatients, geriatric patients, patients with neuromusculardisease, burns, end-stage renal disease, and patientsundergoing coronary artery bypass graft surgery withinduced hypothermia ( 2.2, 2.3, 2.4, 2.5)
○ Confusion infusion rate ( 2.6)
○ Preparation instructions ( 2.7)
○ Drug compatibility ( 2.8)