MARINOL
These highlights do not include all the information needed to use MARINOL® safely and effectively. See full prescribing information for MARINOL. MARINOL (dronabinol) capsules, for oral use, CIII Initial U.S. Approval: 1985
d0efeeec-640d-43c3-8f0a-d31324a11c68
HUMAN PRESCRIPTION DRUG LABEL
Feb 14, 2023
ThePharmaNetwork, LLC
DUNS: 939435280
Products 3
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Dronabinol
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (7)
Dronabinol
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (7)
Dronabinol
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (5)
Drug Labeling Information
WARNINGS AND PRECAUTIONS SECTION
5 WARNINGS AND PRECAUTIONS
5.1 Neuropsychiatric Adverse Reactions
Psychiatric Adverse Reactions
Dronabinol has been reported to exacerbate mania, depression, or schizophrenia. Significant CNS symptoms followed oral doses of 0.4 mg/kg (28 mg per 70 kg patient) of MARINOL in antiemetic studies.
Prior to initiating treatment with MARINOL, screen patients for a history of these illnesses. Avoid use in patients with a psychiatric history or, if the drug cannot be avoided, monitor patients for new or worsening psychiatric symptoms during treatment. Also, avoid concomitant use with other drugs that are associated with similar psychiatric effects.
Cognitive Adverse Reactions
Use of MARINOL has been associated with cognitive impairment and altered mental state. Reduce the dose of MARINOL or discontinue use of MARINOL if signs or symptoms of cognitive impairment develop. Elderly patients may be more sensitive to the neurological and psychoactive effects of MARINOL [see Use in Specific Populations (8.4, 8.5)].
Hazardous Activities
MARINOL can cause and may impair the mental and/or physical abilities required for the performance of hazardous tasks such as driving a motor vehicle or operating machinery. Concomitant use of other drugs that cause dizziness, confusion, sedation, or somnolence such as CNS depressants may increase this effect (e.g., barbiturates, benzodiazepines, ethanol, lithium, opioids, buspirone, scopolamine, antihistamines, tricyclic antidepressants, other anticholinergic agents, muscle relaxants). Inform patients not to operate motor vehicles or other dangerous machinery until they are reasonably certain that MARINOL does not affect them adversely.
5.2 Hemodynamic Instability
Patients may experience occasional hypotension, possible hypertension, syncope, or tachycardia while taking MARINOL [see Clinical Pharmacology (12.2)]. Patients with cardiac disorders may be at higher risk. Avoid concomitant use of other drugs that are also associated with similar cardiac effects (e.g., amphetamines, other sympathomimetic agents, atropine, amoxapine, scopolamine, antihistamines, other anticholinergic agents, amitriptyline, desipramine, other tricyclic antidepressants). Monitor patients for changes in blood pressure, heart rate, and syncope after initiating or increasing the dosage of MARINOL.
5.3 Seizures
Seizure and seizure-like activity have been reported in patients receiving dronabinol. Weigh this potential risk against the benefits before prescribing MARINOL to patients with a history of seizures, including those receiving anti-epileptic medication or with other factors that can lower the seizure threshold. Monitor patients with a history of seizure disorders for worsened seizure control during MARINOL therapy.
If a seizure occurs, advise patients to discontinue MARINOL and contact a healthcare provider immediately.
5.4 Multiple Substance Abuse
Patients with a history of substance abuse or dependence, including marijuana or alcohol, may be more likely to abuse MARINOL as well.
Assess each patient’s risk for abuse or misuse prior to prescribing MARINOL and monitor patients with a history of substance abuse during treatment with MARINOL for the development of these behaviors or conditions.
5.5 Paradoxical Nausea, Vomiting, or Abdominal Pain
Nausea, vomiting, or abdominal pain can occur during treatment with synthetic delta-9- tetrahydrocannabinol (delta-9-THC), the active ingredient in MARINOL® (dronabinol capsules, USP). In some cases, these adverse reactions were severe (e.g., dehydration, electrolyte abnormalities) and required dose reduction or drug discontinuation. Symptoms are similar to cannabinoid hyperemesis syndrome (CHS), which is described as cyclical events of abdominal pain, nausea, and vomiting in chronic, long-term users of delta-9-THC products.
Because patients may not recognize these symptoms as abnormal, it is important to specifically ask patients or their caregivers about the development of worsening of nausea, vomiting, or abdominal pain while being treated with MARINOL. Consider dose reduction or discontinuing MARINOL if a patient develops worsening nausea, vomiting, or abdominal pain while on treatment.
- Neuropsychiatric Adverse Reactions: May cause psychiatric and cognitive effects and impair mental and/or physical abilities. Avoid use in patients with a psychiatric history. Monitor for symptoms and avoid concomitant use of drugs with similar effects. Inform patients not to operate motor vehicles or other dangerous machinery until they are reasonably certain that MARINOL® (dronabinol capsules, USP), does not affect them adversely. (5.1)
- Hemodynamic Instability: Patients with cardiac disorders may experience hypotension, hypertension, syncope or tachycardia. Avoid concomitant use of drugs with similar effects and monitor for hemodynamic changes after initiating or increasing the dosage of MARINOL. (5.2)
- Seizures and Seizure-like Activity: Weigh the potential risk versus benefits before prescribing MARINOL to patients with a history of seizures, including those requiring anti-epileptic medication or with other factors that lower the seizure threshold. Monitor patients and discontinue if seizures occur. (5.3)
- Multiple Substance Abuse: Assess risk for abuse or misuse in patients with a history of substance abuse or dependence, prior to prescribing MARINOL and monitor for the development of associated behaviors or conditions. (5.4)
- Paradoxical Nausea, Vomiting, or Abdominal Pain: Consider dose reduction or discontinuation, if worsening of symptoms while on treatment. (5.5)
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
7.1 Additive CNS Effects
Additive CNS effects (e.g., dizziness, confusion, sedation, somnolence) may occur when MARINOL is taken concomitantly with drugs that have similar effects on the central nervous system such as CNS depressants [see Warnings and Precautions (5.1)].
7.2 Additive Cardiac Effects
Additive cardiac effects (e.g., hypotension, hypertension, syncope, tachycardia) may occur when MARINOL is taken concomitantly with drugs that have similar effects on the cardiovascular system [see Warnings and Precautions (5.2)].
7.3 Effect of Other Drugs on Dronabinol
Dronabinol is primarily metabolized by CYP2C9 and CYP3A4 enzymes based on published in vitro studies. Inhibitors of these enzymes may increase, while inducers may decrease, the systemic exposure of dronabinol and/or its active metabolite resulting in an increase in dronabinol-related adverse reactions or loss of efficacy of MARINOL.
Monitor for potentially increased dronabinol-related adverse reactions when MARINOL is co-administered with inhibitors of CYP2C9 (e.g., amiodarone, fluconazole) and inhibitors of CYP3A4 enzymes (e.g., ketoconazole, itraconazole, clarithromycin, ritonavir, erythromycin, grapefruit juice).
7.4 Highly Protein-Bound Drugs
Dronabinol is highly bound to plasma proteins, and therefore, might displace and increase the free fraction of other concomitantly administered protein- bound drugs.
Although this displacement has not been confirmed in vivo, monitor patients for increased adverse reactions to narrow therapeutic index drugs that are highly protein-bound (e.g., warfarin, cyclosporine, amphotericin B) when initiating treatment or increasing the dosage of MARINOL.
- Inhibitors and inducers of CYP2C9 and CYP3A4: May alter dronabinol systemic exposure; monitor for potential dronabinol-related adverse reactions or loss of efficacy. (7.3)
- Highly protein-bound drugs: Potential for displacement of other drugs from plasma proteins; monitor for adverse reactions to concomitant highly protein-bound drugs and narrow therapeutic index drugs (e.g., warfarin, cyclosporine, amphotericin B) when initiating or increasing the dosage of MARINOL. (7.4)
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Anorexia Associated with Weight Loss in Adult Patients with AIDS
Starting Dosage
The recommended adult starting dosage of MARINOL is 2.5 mg orally twice daily,
one hour before lunch and dinner.
In elderly patients or patients unable to tolerate 2.5 mg twice daily,
consider initiating MARINOL at 2.5 mg once daily one hour before dinner or at
bedtime to reduce the risk of central nervous system (CNS) symptoms [see Use in Specific Populations (8.5)].
Dosing later in the day may reduce the frequency of CNS adverse reactions. CNS
adverse reactions are dose-related [see Warnings and Precautions (5.1)];
therefore monitor patients and reduce the dosage as needed. If CNS adverse
reactions of feeling high, dizziness, confusion, and somnolence occur, they
usually resolve in 1 to 3 days and usually do not require dosage reduction. If
CNS adverse reactions are severe or persistent, reduce the dosage to 2.5 mg in
the evening or at bedtime.
Dosage Titration
If tolerated and further therapeutic effect is desired, the dosage may be
increased gradually to 2.5 mg one hour before lunch and 5 mg one hour before
dinner. Increase the dose of MARINOL gradually in order to reduce the
frequency of dose-related adverse reactions [see Warnings and Precautions (5.1)].
Most patients respond to 2.5 mg twice daily, but the dose may be further
increased to 5 mg one hour before lunch and 5 mg one hour before dinner, as
tolerated to achieve a therapeutic effect.
Maximum Dosage: 10 mg twice daily.
2.2 Nausea and Vomiting Associated with Cancer Chemotherapy in Adult
Patients Who Failed Conventional Antiemetics
Starting Dosage
The recommended starting dosage of MARINOL is 5 mg/m2, orally administered 1 to 3 hours prior to the administration of chemotherapy and then every 2 to 4 hours after chemotherapy, for a total of 4 to 6 doses per day.
In elderly patients, consider initiating MARINOL at 2.5 mg/m2 once daily 1 to 3 hours prior to chemotherapy to reduce the risk of CNS symptoms [see Use in Specific Populations (8.5)].
Administer the first dose on an empty stomach at least 30 minutes before eating. Subsequent doses can be taken without regard to meals [see Clinical Pharmacology (12.3)].
The timing of dosing in relation to meal times should be kept consistent for each chemotherapy cycle, once the dosage has been determined from the titration process.
Dosage Titration
The dosage can be titrated to clinical response during a chemotherapy cycle or subsequent cycles, based upon initial response, as tolerated to achieve a clinical effect, in increments of 2.5 mg/m2.
The maximum dosage is 15 mg/m2 per dose for 4 to 6 doses per day.
Adverse reactions are dose-related and psychiatric symptoms increase significantly at the maximum dosage [see Warnings and Precautions (5.1)]. Monitor patients for adverse reactions and consider decreasing the dose to 2.5 mg once daily 1 to 3 hours prior to chemotherapy to reduce the risk of CNS adverse reactions.
Anorexia Associated with Weight Loss in Adult Patients with AIDS (2.1):
- The recommended adult starting dosage is 2.5 mg orally twice daily, one hour before lunch and dinner.
- See the full prescribing information for dosage titration to manage adverse reactions and to achieve desired therapeutic effect.
Nausea and Vomiting Associated with Chemotherapy in Adult Patients Who Failed Conventional Antiemetics (2.2):
- The recommended starting dosage is 5 mg/m2, administered 1 to 3 hours prior to the administration of chemotherapy, then every 2 to 4 hours after chemotherapy, for a total of 4 to 6 doses per day. Administer the first dose on an empty stomach at least 30 minutes prior to eating; subsequent doses can be taken without regard to meals.
- See the full prescribing information for dosage titration to manage adverse reactions and to achieve desired therapeutic effect.
DRUG ABUSE AND DEPENDENCE SECTION
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
MARINOL contains dronabinol capsules, a Schedule III controlled substance.
9.2 Abuse
MARINOL contains dronabinol, the main psychoactive component in marijuana. Ingestion of high doses of dronabinol increases the risk of psychiatric adverse reactions if abused or misused, while continued administration can lead to addiction. Psychiatric adverse reactions may include psychosis, hallucinations, depersonalization, mood alteration, and paranoia.
In an open-label study in patients with AIDS who received MARINOL for up to five months, no abuse, diversion or systematic change in personality or social functioning were observed despite the inclusion of a substantial number of patients with a past history of drug abuse.
Patients should be instructed to keep MARINOL in a secure place out of reach of others for whom the medication has not been prescribed.
9.3 Dependence
Physical dependence is a state that develops as a result of physiological adaptation in response to repeated drug use. Physical dependence manifests by drug class-specific withdrawal symptoms after abrupt discontinuation or a significant dose reduction of a drug. The appearance of a withdrawal syndrome when administration of the drug is terminated is the only actual evidence of physical dependence. Physical dependence can develop during chronic therapy with MARINOL, and develops after chronic abuse of marijuana.
A withdrawal syndrome was reported after the abrupt discontinuation of dronabinol in subjects receiving dosages of 210 mg per day for 12 to 16 consecutive days. Within 12 hours after discontinuation, subjects manifested symptoms such as irritability, insomnia, and restlessness. By approximately 24 hours post-dronabinol discontinuation, withdrawal symptoms intensified to include “hot flashes,” sweating, rhinorrhea, loose stools, hiccoughs, and anorexia. These withdrawal symptoms gradually dissipated over the next 48 hours.
Electroencephalographic changes consistent with the effects of drug withdrawal (hyperexcitation) were recorded in patients after abrupt dechallenge. Patients also complained of disturbed sleep for several weeks after discontinuing therapy with high dosages of dronabinol.
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In 2-year carcinogenicity studies, there was no evidence of carcinogenicity in rats at doses up to 50 mg/kg/day dronabinol (approximately 20 times the MRHD in AIDS patients on a body surface area basis) or in mice at doses up to 500 mg/kg/day (approximately 100 times the MRHD in AIDS patients on a body surface area basis).
Dronabinol was not genotoxic in the Ames tests, the in vitro chromosomal aberration test in Chinese hamster ovary cells, and the in vivo mouse micronucleus test. However, dronabinol produced a weak positive response in a sister chromatid exchange test in Chinese hamster ovary cells.
In a long-term study (77 days) in rats, oral administration of dronabinol at doses of 30 to 150 mg/m2, equivalent to 2 to 10 times the MRHD of 15 mg/m2/day in AIDS patients or 0.3 to 1.5 times the MRHD of 90 mg/m2/day in cancer patients, reduced ventral prostate, seminal vesicle and epididymal weights and caused a decrease in seminal fluid volume. Decreases in spermatogenesis, number of developing germ cells, and number of Leydig cells in the testis were also observed. However, sperm count, mating success, and testosterone levels were not affected. The significance of these animal findings in humans is not known.
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
The effectiveness of MARINOL has been established based on studies for the treatment of anorexia associated with weight loss in patients with AIDS and nausea and vomiting associated with cancer chemotherapy in patients who have failed to respond adequately to conventional antiemetic treatments.
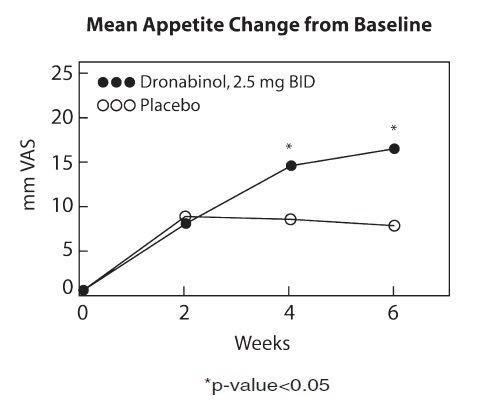
14.1 Appetite Stimulation
The appetite stimulant effect of MARINOL in the treatment of AIDS-related anorexia associated with weight loss was studied in a randomized, double- blind, placebo-controlled study involving 139 patients. The initial dosage of MARINOL in all patients was 5 mg/day, administered in doses of 2.5 mg one hour before lunch and one hour before dinner. In pilot studies, early morning administration of MARINOL appeared to have been associated with an increased frequency of adverse experiences, as compared to dosing later in the day. The effect of MARINOL on appetite, weight, mood, and nausea was measured at scheduled intervals during the six-week treatment period. Side effects (feeling high, dizziness, confusion, somnolence) occurred in 13 of 72 patients (18%) at this dosage level and the dosage was reduced to 2.5 mg/day, administered as a single dose at supper or bedtime.
Of the 112 patients that completed at least 2 visits in the randomized, double-blind, placebo-controlled study, 99 patients had appetite data at 4-weeks (50 received MARINOL and 49 received placebo) and 91 patients had appetite data at 6-weeks (46 received MARINOL and 45 received placebo). A statistically significant difference between MARINOL and placebo was seen in appetite as measured by the visual analog scale at weeks 4 and 6 (see figure). Trends toward improved body weight and mood, and decreases in nausea were also seen.
After completing the 6-week study, patients were allowed to continue treatment with MARINOL in an open-label study, in which there was a sustained improvement in appetite.