
Sandimmune
Soft Gelatin Capsules Oral Solution Injection
5e5926a7-1de0-4b54-a5c0-286b6200ff82
HUMAN PRESCRIPTION DRUG LABEL
Aug 12, 2025
Novartis Pharmaceuticals Corporation
DUNS: 002147023
Products 4
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
cyclosporine
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (4)
cyclosporine
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (10)
cyclosporine
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (3)
cyclosporine
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (10)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
PRINCIPAL DISPLAY PANEL
NDC 0078-0109-01
Sandimmune® Injection
(cyclosporine injection, USP)
Sterile solution for intravenous infusion only
Rx only
FOR INFUSION ONLY. DILUTE BEFORE USE.
250 mg (5 mL ampul)
10 Ampuls
NOVARTIS
DRUG INTERACTIONS SECTION
Drug Interactions
A. Effect of Drugs and Other Agents on Cyclosporine Pharmacokinetics and/or Safety
All of the individual drugs cited below are well substantiated to interact with cyclosporine. In addition, concomitant use of nonsteroidal anti- inflammatory drugs (NSAIDs) with cyclosporine, particularly in the setting of dehydration, may potentiate renal dysfunction. Caution should be exercised when using other drugs which are known to impair renal function (see WARNINGS, Nephrotoxicity).
Drugs That May Potentiate Renal Dysfunction
|
Antibiotics |
Antineoplastic |
Antifungals |
Anti-Inflammatory Drugs |
Gastrointestinal Agents |
Immunosuppressives |
Other Drugs |
|
ciprofloxacin |
melphalan |
amphotericin B |
azapropazon |
cimetidine |
tacrolimus |
fibric acid derivatives |
|
gentamicin |
ketoconazole |
colchicine |
ranitidine |
methotrexate | ||
|
tobramycin |
diclofenac | |||||
|
trimethoprim |
naproxen | |||||
|
vancomycin |
sulindac |
During the concomitant use of a drug that may exhibit additive or synergistic renal impairment potential with cyclosporine, close monitoring of renal function (in particular serum creatinine) should be performed. If a significant impairment of renal function occurs, reduction in the dosage of cyclosporine and/or coadministered drug or an alternative treatment should be considered.
Cyclosporine is extensively metabolized by CYP 3A isoenzymes, in particular CYP3A4, and is a substrate of the multidrug efflux transporter P-glycoprotein. Various agents are known to either increase or decrease plasma or whole blood concentrations of cyclosporine usually by inhibition or induction of CYP3A4 or P-glycoprotein transporter or both. Compounds that decrease cyclosporine absorption, such as orlistat, should be avoided. Appropriate Sandimmune (cyclosporine) dosage adjustment to achieve the desired cyclosporine concentrations is essential when drugs that significantly alter cyclosporine concentrations are used concomitantly (see DOSAGE AND ADMINISTRATION, Blood Concentration Monitoring).
** 1. Drugs ThatIncrease Cyclosporine Concentrations**
|
Calcium Channel Blockers |
Antifungals |
Antibiotics |
Glucocorticoids |
Other Drugs |
|
diltiazem |
fluconazole |
azithromycin |
methylprednisolone |
allopurinol |
|
nicardipine |
itraconazole |
clarithromycin |
amiodarone | |
|
verapamil |
ketoconazole |
erythromycin |
bromocriptine | |
|
voriconazole |
quinupristin/ |
colchicine | ||
|
danazol | ||||
|
imatinib | ||||
|
metoclopramide | ||||
|
nefazodone | ||||
|
oral contraceptives |
HIV Protease inhibitors
The HIV protease inhibitors (e.g., indinavir, nelfinavir, ritonavir, and saquinavir) are known to inhibit cytochrome P-450 3A and thus could potentially increase the concentrations of cyclosporine, however, no formal studies of the interaction are available. Care should be exercised when these drugs are administered concomitantly.
Grapefruit Juice
Grapefruit and grapefruit juice affect metabolism, increasing blood concentrations of cyclosporine, thus should be avoided.
** 2. Drugs/Dietary Supplements ThatDecrease Cyclosporine Concentrations**
|
Antibiotics |
Anticonvulsants |
Other Drugs / Dietary Supplements | |
|
nafcillin |
carbamazepine |
bosentan |
St. John’s Wort |
|
rifampin |
oxcarbazepine |
octreotide | |
|
phenobarbital |
orlistat | ||
|
phenytoin |
sulfinpyrazone | ||
|
terbinafine | |||
|
ticlopidine |
Bosentan
Coadministration of bosentan (250 to 1000 mg every 12 hours based on tolerability) and cyclosporine (300 mg every 12 hours for 2 days then dosing to achieve a Cmin of 200 to 250 ng/mL) for 7 days in healthy subjects resulted in decreases in the cyclosporine mean dose-normalized AUC, Cmax, and trough concentration of approximately 50%, 30% and 60%, respectively, compared to when cyclosporine was given alone (see also Effect of Cyclosporine on the Pharmacokinetics and/or Safety of Other Drugs or Agents). Coadministration of cyclosporine with bosentan should be avoided.
Boceprevir
Coadministration of boceprevir (800 mg three times daily for 7 days) and cyclosporine (100 mg single dose) in healthy subjects resulted in increases in the mean AUC and Cmax of cyclosporine approximately 2.7-fold and 2-fold, respectively, compared to when cyclosporine was given alone.
Telaprevir
Coadministration of telaprevir (750 mg every 8 hours for 11 days) with cyclosporine (10 mg on Day 8) in healthy subjects resulted in increases in the mean dose-normalized AUC and Cmax of cyclosporine approximately 4.5-fold and 1.3-fold, respectively, compared to when cyclosporine (100 mg single dose) was given alone.
St. John’s Wort
There have been reports of a serious drug interaction between cyclosporine and the herbal dietary supplement, St. John’s Wort. This interaction has been reported to produce a marked reduction in the blood concentrations of cyclosporine, resulting in subtherapeutic levels, rejection of transplanted organs, and graft loss.
Rifabutin
Rifabutin is known to increase the metabolism of other drugs metabolized by the cytochrome P-450 system. The interaction between rifabutin and cyclosporine has not been studied. Care should be exercised when these two drugs are administered concomitantly.
B. Effect of Cyclosporine on the Pharmacokinetics and/or Safety of Other Drugs or Agents
Cyclosporine is an inhibitor of CYP3A4 and of multiple drug efflux transporters (e.g., P-glycoprotein) and may increase plasma concentrations of comedications that are substrates of CYP3A4, P-glycoprotein, or organic anion transporter proteins.
Cyclosporine may reduce the clearance of digoxin, colchicine, prednisolone, HMG-CoA reductase inhibitors (statins) and aliskiren, bosentan, dabigatran, repaglinide, NSAIDs, sirolimus, etoposide, and other drugs.
See the full prescribing information of the other drug for further information and specific recommendations. The decision on coadministration of cyclosporine with other drugs or agents should be made by the healthcare provider following the careful assessment of benefits and risks.
Digoxin
Severe digitalis toxicity has been seen within days of starting cyclosporine in several patients taking digoxin. If digoxin is used concurrently with cyclosporine, serum digoxin concentrations should be monitored.
Colchicine
There are reports on the potential of cyclosporine to enhance the toxic effects of colchicine, such as myopathy and neuropathy, especially in patients with renal dysfunction. Concomitant administration of cyclosporine and colchicine results in significant increases in colchicine plasma concentrations. If colchicine is used concurrently with cyclosporine, a reduction in the dosage of colchicine is recommended.
HMG Co-A Reductase Inhibitors (Statins)
Literature and postmarketing cases of myotoxicity, including muscle pain and weakness, myositis, and rhabdomyolysis, have been reported with concomitant administration of cyclosporine with lovastatin, simvastatin, atorvastatin, pravastatin, and rarely, fluvastatin. When concurrently administered with cyclosporine, the dosage of these statins should be reduced according to label recommendations. Statin therapy needs to be temporarily withheld or discontinued in patients with signs and symptoms of myopathy or those with risk factors predisposing to severe renal injury, including renal failure, secondary to rhabdomyolysis.
Repaglinide
Cyclosporine may increase the plasma concentrations of repaglinide and thereby increase the risk of hypoglycemia. In 12 healthy male subjects who received two doses of 100 mg cyclosporine capsule orally 12 hours apart with a single dose of 0.25 mg repaglinide tablet (one half of a 0.5 mg tablet) orally 13 hours after the cyclosporine initial dose, the repaglinide mean Cmax and AUC were increased 1.8-fold (range, 0.6 to 3.7-fold) and 2.4-fold (range, 1.2 to 5.3-fold), respectively. Close monitoring of blood glucose level is advisable for a patient taking cyclosporine and repaglinide concomitantly.
Ambrisentan
Coadministration of ambrisentan (5 mg daily) and cyclosporine (100 to 150 mg twice daily initially, then dosing to achieve Cmin 150 to 200 ng/mL) for 8 days in healthy subjects resulted mean increases in ambrisentan AUC and Cmax of approximately 2-fold and 1.5-fold, respectively, compared to ambrisentan alone. When coadministering ambrisentan with cyclosporine, the ambrisentan dose should not be titrated to the recommended maximum daily dose.
Anthracycline Antibiotics
High doses of cyclosporine (e.g., at starting intravenous dose of 16 mg/kg/day) may increase the exposure to anthracycline antibiotics (e.g., doxorubicin, mitoxantrone, daunorubicin) in cancer patients.
Aliskiren
Cyclosporine alters the pharmacokinetics of aliskiren, a substrate of P-glycoprotein and CYP3A4. In 14 healthy subjects who received concomitantly single doses of cyclosporine (200 mg) and reduced dose aliskiren (75 mg), the mean Cmax of aliskiren was increased by approximately 2.5-fold (90% CI: 1.96 to 3.17) and the mean AUC by approximately 4.3-fold (90% CI: 3.52 to 5.21), compared to when these subjects received aliskiren alone. The concomitant administration of aliskiren with cyclosporine prolonged the median aliskiren elimination half-life (26 hours versus 43 to 45 hours) and the Tmax (0.5 hours versus 1.5 to 2.0 hours). The mean AUC and Cmax of cyclosporine were comparable to reported literature values. Coadministration of cyclosporine and aliskiren in these subjects also resulted in an increase in the number and/or intensity of adverse events, mainly headache, hot flush, nausea, vomiting, and somnolence. The coadministration of cyclosporine with aliskiren is not recommended.
Bosentan
In healthy subjects, coadministration of bosentan and cyclosporine resulted in time-dependent mean increases in dose-normalized bosentan trough concentrations (i.e., approximately 21-fold on Day 1 and 2-fold on Day 8 (steady state)) compared to when bosentan was given alone as a single dose on Day 1 (see also Effect of Drugs and Other Agents on Cyclosporine Pharmacokinetics and/or Safety). Coadministration of cyclosporine with bosentan should be avoided.
Dabigatran
The effect of cyclosporine on dabigatran concentrations had not been formally studied. Concomitant administration of dabigatran and cyclosporine may result in increased plasma dabigatran concentrations due to the P-gp inhibitory activity of cyclosporine. Coadministration of cyclosporine with dabigatran should be avoided.
Potassium Sparing Diuretics
Cyclosporine should not be used with potassium-sparing diuretics because hyperkalemia can occur. Caution is also required when cyclosporine is coadministered with potassium-sparing drugs (e.g., angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists), potassium-containing drugs as well as in patients on a potassium-rich diet. Control of potassium levels in these situations is advisable.
Nonsteroidal Anti-inflammatory Drug (NSAID) Interactions
Clinical status and serum creatinine should be closely monitored when cyclosporine is used with NSAIDs in rheumatoid arthritis patients (see WARNINGS).
Pharmacodynamic interactions have been reported to occur between cyclosporine and both naproxen and sulindac, in that concomitant use is associated with additive decreases in renal function, as determined by 99mTc- diethylenetriaminepenta acetic acid (DTPA) and (p-aminohippuric acid) PAH clearances. Although concomitant administration of diclofenac does not affect blood concentrations of cyclosporine, it has been associated with approximate doubling of diclofenac blood levels and occasional reports of reversible decreases in renal function. Consequently, the dose of diclofenac should be in the lower end of the therapeutic range.
Methotrexate Interaction
Preliminary data indicate that when methotrexate and cyclosporine were coadministered to rheumatoid arthritis patients (N = 20), methotrexate concentrations (AUCs) were increased approximately 30% and the concentrations (AUCs) of its metabolite, 7-hydroxy methotrexate, were decreased by approximately 80%. The clinical significance of this interaction is not known. Cyclosporine concentrations do not appear to have been altered (N = 6).
Sirolimus
Elevations in serum creatinine were observed in studies using sirolimus in combination with full-dose cyclosporine. This effect is often reversible with cyclosporine dose reduction. Simultaneous coadministration of cyclosporine significantly increases blood levels of sirolimus. To minimize increases in sirolimus blood concentrations, it is recommended that sirolimus be given 4 hours after cyclosporine administration.
Nifedipine
Frequent gingival hyperplasia when nifedipine is given concurrently with cyclosporine has been reported. The concomitant use of nifedipine should be avoided in patients in whom gingival hyperplasia develops as a side effect of cyclosporine.
Methylprednisolone
Convulsions when high dose methylprednisolone is given concomitantly with cyclosporine have been reported.
Other Immunosuppressive Drugs and Agents
Psoriasis patients receiving other immunosuppressive agents or radiation therapy (including PUVA and UVB) should not receive concurrent cyclosporine because of the possibility of excessive immunosuppression.
Interactions Resulting in Decrease of Other Drug Levels
Cyclosporine inhibits the enterohepatic circulation of mycophenolic acid (MPA). Concomitant administration of cyclosporine and mycophenolate mofetil or mycophenolate sodium in transplant patients may decrease the mean exposure of MPA by 20% to 50% when compared with other immunosuppressants, which could reduce efficacy of mycophenolate mofetil or mycophenolate sodium. Monitor patients for alterations in efficacy of mycophenolate mofetil or mycophenolate sodium, when they are coadministered with cyclosporine.
C. Effect of Cyclosporine on the Efficacy of Live Vaccines
During treatment with cyclosporine, vaccination may be less effective. The use of live vaccines should be avoided.
For additional information on Cyclosporine Drug Interactions please contact Novartis Medical Affairs Department at 1-888-NOW-NOVA (1-888-669-6682).
DOSAGE & ADMINISTRATION SECTION
DOSAGE AND ADMINISTRATION
**Sandimmune Soft Gelatin Capsules (cyclosporine capsules, USP) and
Sandimmune Oral Solution (cyclosporine oral solution, USP)**
Sandimmune Soft Gelatin Capsules (cyclosporine capsules, USP) and Sandimmune Oral Solution (cyclosporine oral solution, USP) have decreased bioavailability in comparison to Neoral Soft Gelatin Capsules (cyclosporine capsules, USP) MODIFIED and Neoral Oral Solution (cyclosporine oral solution, USP) MODIFIED. Sandimmune and Neoral are not bioequivalent and cannot be used interchangeably without physician supervision.
The initial oral dose of Sandimmune (cyclosporine) should be given 4 to 12 hours prior to transplantation as a single dose of 15 mg/kg. Although a daily single dose of 14 to 18 mg/kg was used in most clinical trials, few centers continue to use the highest dose, most favoring the lower end of the scale. There is a trend towards use of even lower initial doses for renal transplantation in the ranges of 10 to 14 mg/kg/day. The initial single daily dose is continued postoperatively for 1 to 2 weeks and then tapered by 5% per week to a maintenance dose of 5 to 10 mg/kg/day. Some centers have successfully tapered the maintenance dose to as low as 3 mg/kg/day in selected renal transplant patients without an apparent rise in rejection rate.
See Blood Concentration Monitoring, below.
Specific Populations
Renal Impairment
Cyclosporine undergoes minimal renal elimination and its pharmacokinetics do not appear to be significantly altered in patients with end-stage renal disease who receive routine hemodialysis treatments (see CLINICAL PHARMACOLOGY). However, due to its nephrotoxic potential (see WARNINGS), careful monitoring of renal function is recommended; cyclosporine dosage should be reduced if indicated (see WARNINGS and PRECAUTIONS).
Hepatic Impairment
The clearance of cyclosporine may be significantly reduced in severe liver disease patients (see CLINICAL PHARMACOLOGY). Dose reduction may be necessary in patients with severe liver impairment to maintain blood concentrations within the recommended target range (see WARNINGS and PRECAUTIONS).
Pediatrics
In pediatric usage, the same dose and dosing regimen may be used as in adults although in several studies, children have required and tolerated higher doses than those used in adults.
Adjunct therapy with adrenal corticosteroids is recommended. Different tapering dosage schedules of prednisone appear to achieve similar results. A dosage schedule based on the patient’s weight started with 2.0 mg/kg/day for the first 4 days tapered to 1.0 mg/kg/day by 1 week, 0.6 mg/kg/day by 2 weeks, 0.3 mg/kg/day by 1 month, and 0.15 mg/kg/day by 2 months and thereafter as a maintenance dose. Another center started with an initial dose of 200 mg tapered by 40 mg/day until reaching 20 mg/day. After 2 months at this dose, a further reduction to 10 mg/day was made. Adjustments in dosage of prednisone must be made according to the clinical situation.
To make Sandimmune Oral Solution (cyclosporine oral solution, USP) more palatable, the oral solution may be diluted with milk, chocolate milk, or orange juice preferably at room temperature. Patients should avoid switching diluents frequently. Sandimmune Soft Gelatin Capsules and Oral Solution should be administered on a consistent schedule with regard to time of day and relation to meals.
Take the prescribed amount of Sandimmune (cyclosporine) from the container using the dosage syringe supplied after removal of the protective cover, and transfer the solution to a glass of milk, chocolate milk, or orange juice. Stir well and drink at once. Do not allow to stand before drinking. It is best to use a glass container and rinse it with more diluent to ensure that the total dose is taken. After use, replace the dosage syringe in the protective cover. Do not rinse the dosage syringe with water or other cleaning agents either before or after use. If the dosage syringe requires cleaning, it must be completely dry before resuming use. Introduction of water into the product by any means will cause variation in dose.
Sandimmune**®**** Injection (cyclosporine injection, USP)**
FOR INFUSION ONLY
Note: Anaphylactic reactions have occurred with Sandimmune Injection (cyclosporine injection, USP). See WARNINGS.
Patients unable to take Sandimmune Soft Gelatin Capsules or Oral Solution pre- or postoperatively may be treated with the intravenous (IV) concentrate. Sandimmune Injection (cyclosporine injection, USP) is administered at 1/3 the oral dose. The initial dose of Sandimmune Injection (cyclosporine injection, USP) should be given 4 to 12 hours prior to transplantation as a single intravenous dose of 5 to 6 mg/kg/day. This daily single dose is continued postoperatively until the patient can tolerate the soft gelatin capsules or oral solution. Patients should be switched to Sandimmune Soft Gelatin Capsules or Oral Solution as soon as possible after surgery. In pediatric usage, the same dose and dosing regimen may be used, although higher doses may be required.
Adjunct steroid therapy is to be used (See aforementioned).
Immediately before use, the intravenous concentrate should be diluted 1 mL Sandimmune Injection (cyclosporine injection, USP) in 20 mL to 100 mL 0.9% Sodium Chloride Injection or 5% Dextrose Injection using appropriate aseptic technique and given in a slow intravenous infusion over 2 to 6 hours.
Based on the chemical and physical in-use stability data, the infusion should be completed within 6 hours at room temperature. Discard any unused diluted solution. If not administered immediately, the diluted solution can be stored at 2°C to 8°C (under refrigeration), provided that the total duration for both storage and infusion is less than 24 hours.
The Cremophor® EL (polyoxyethylated castor oil) contained in the concentrate for intravenous infusion can cause phthalate stripping from PVC.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Blood Concentration Monitoring
Several study centers have found blood concentration monitoring of cyclosporine useful in patient management. While no fixed relationships have yet been established, in one series of 375 consecutive cadaveric renal transplant recipients, dosage was adjusted to achieve specific whole blood 24-hour trough concentrations of 100 to 200 ng/mL as determined by high- pressure liquid chromatography (HPLC).
Of major importance to blood concentration analysis is the type of assay used. The above concentrations are specific to the parent cyclosporine molecule and correlate directly to the new monoclonal specific radioimmunoassays (mRIA-sp). Nonspecific assays are also available which detect the parent compound molecule and various of its metabolites. Older studies often cited concentrations using a nonspecific assay which were roughly twice those of specific assays. Assay results are not interchangeable and their use should be guided by their approved labeling. If plasma specimens are employed, concentrations will vary with the temperature at the time of separation from whole blood. Plasma concentrations may range from 1/2 to 1/5 of whole blood concentrations. Refer to individual assay labeling for complete instructions. In addition, Transplantation Proceedings (June 1990) contains position papers and a broad consensus generated at the Cyclosporine-Therapeutic Drug Monitoring conference that year. Blood concentration monitoring is not a replacement for renal function monitoring or tissue biopsies.
CLINICAL PHARMACOLOGY SECTION
CLINICAL PHARMACOLOGY
Cyclosporine is a potent immunosuppressive agent, which in animals prolongs survival of allogeneic transplants involving skin, heart, kidney, pancreas, bone marrow, small intestine, and lung. Cyclosporine has been demonstrated to suppress some humoral immunity and to a greater extent, cell-mediated reactions, such as allograft rejection, delayed hypersensitivity, experimental allergic encephalomyelitis, Freund’s adjuvant arthritis, and graft vs. host disease in many animal species for a variety of organs.
Successful kidney, liver, and heart allogeneic transplants have been performed in man using cyclosporine.
The exact mechanism of action of cyclosporine is not known. Experimental evidence suggests that the effectiveness of cyclosporine is due to specific and reversible inhibition of immunocompetent lymphocytes in the G0- or G1-phase of the cell cycle. T-lymphocytes are preferentially inhibited. The T-helper cell is the main target, although the T-suppressor cell may also be suppressed. Cyclosporine also inhibits lymphokine production and release, including interleukin-2 or T-cell growth factor (TCGF).
No functional effects on phagocytic (changes in enzyme secretions not altered, chemotactic migration of granulocytes, macrophage migration, carbon clearance in vivo) or tumor cells (growth rate, metastasis) can be detected in animals. Cyclosporine does not cause bone marrow suppression in animal models or man.
The absorption of cyclosporine from the gastrointestinal tract is incomplete and variable. Peak concentrations (Cmax) in blood and plasma are achieved at about 3.5 hours. Cmax and area under the plasma or blood concentration/time curve (AUC) increase with the administered dose; for blood, the relationship is curvilinear (parabolic) between 0 and 1400 mg. As determined by a specific assay, Cmax is approximately 1.0 ng/mL/mg of dose for plasma and 2.7 to 1.4 ng/mL/mg of dose for blood (for low to high doses). Compared to an intravenous infusion, the absolute bioavailability of the oral solution is approximately 30% based upon the results in 2 patients. The bioavailability of Sandimmune Soft Gelatin Capsules (cyclosporine capsules, USP) is equivalent to Sandimmune Oral Solution, (cyclosporine oral solution, USP).
Cyclosporine is distributed largely outside the blood volume. In blood, the distribution is concentration dependent. Approximately 33% to 47% is in plasma, 4% to 9% in lymphocytes, 5% to 12% in granulocytes, and 41% to 58% in erythrocytes. At high concentrations, the uptake by leukocytes and erythrocytes becomes saturated. In plasma, approximately 90% is bound to proteins, primarily lipoproteins.
The disposition of cyclosporine from blood is biphasic with a terminal half- life of approximately 19 hours (range, 10 to 27 hours). Elimination is primarily biliary with only 6% of the dose excreted in the urine.
Cyclosporine is extensively metabolized but there is no major metabolic pathway. Only 0.1% of the dose is excreted in the urine as unchanged drug. Of 15 metabolites characterized in human urine, 9 have been assigned structures. The major pathways consist of hydroxylation of the Cγ-carbon of 2 of the leucine residues, Cη-carbon hydroxylation, and cyclic ether formation (with oxidation of the double bond) in the side chain of the amino acid 3-hydroxyl-N,4-dimethyl-L-2-amino-6-octenoic acid and N-demethylation of N-methyl leucine residues. Hydrolysis of the cyclic peptide chain or conjugation of the aforementioned metabolites do not appear to be important biotransformation pathways.
Specific Populations
Renal Impairment
In a study performed in 4 subjects with end-stage renal disease (creatinine clearance < 5 mL/min), an intravenous infusion of 3.5 mg/kg of cyclosporine over 4 hours administered at the end of a hemodialysis session resulted in a mean volume of distribution (Vdss) of 3.49 L/kg and systemic clearance (CL) of 0.369 L/hr/kg. This systemic CL (0.369 L/hr/kg) was approximately two thirds of the mean systemic CL (0.56 L/hr/kg) of cyclosporine in historical control subjects with normal renal function. In 5 liver transplant patients, the mean clearance of cyclosporine on and off hemodialysis was 463 mL/min and 398 mL/min, respectively. Less than 1% of the dose of cyclosporine was recovered in the dialysate.
Hepatic Impairment
Cyclosporine is extensively metabolized by the liver. Since severe hepatic impairment may result in significantly increased cyclosporine exposures, the dosage of cyclosporine may need to be reduced in these patients.
DESCRIPTION SECTION
DESCRIPTION
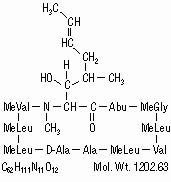
Cyclosporine, the active principle in Sandimmune (cyclosporine) is a cyclic polypeptide immunosuppressant agent consisting of 11 amino acids. It is produced as a metabolite by the fungus species Beauveria nivea.
Chemically, cyclosporine is designated as [R-[R*,R*-(E)]]-cyclic(L-alanyl-D- alanyl-N-methyl-L-leucyl-N-methyl-L-leucyl-N-methyl-L- valyl-3-hydroxy-N,4-dimethyl-L-2-amino-6-octenoyl-L-α-amino-butyryl-N- methylglycyl-N-methyl-L-leucyl-L-valyl-N-methyl-L-leucyl).
Sandimmune**®**** Soft Gelatin Capsules** (cyclosporine capsules, USP) are available in 25 mg and 100 mg strengths.
Each 25 mg capsule contains:
cyclosporine, USP…………………………………………………………………………………………25 mg
alcohol, USP dehydrated………………………………………………………………max 12.7% by volume
Each 100 mg capsule contains:
cyclosporine, USP……………………………………………………………………………………….100 mg
alcohol, USP dehydrated………………………………………………………………max 12.7% by volume
Inactive ingredients: corn oil, gelatin, iron oxide red, linoleoyl macrogolglycerides, sorbitol, and titanium dioxide. May also contain glycerol. 100 mg capsules may contain iron oxide yellow.
Sandimmune**®**** Oral Solution**(cyclosporine oral solution, USP) is available in 50 mL bottles.
Each mL contains:
cyclosporine, USP……………………………………………………………………………………….100 mg
alcohol, Ph. Helv. ……………………………………………………………………………12.5% by volume
dissolved in an olive oil, Ph. Helv./Labrafil M 1944 CS (polyoxyethylated oleic glycerides) vehicle which must be further diluted with milk, chocolate milk, or orange juice before oral administration.
Sandimmune**®**** Injection** (cyclosporine injection, USP) is available in a 5 mL sterile ampul for intravenous (IV) administration.
Each mL contains:
cyclosporine, USP…………………………………………………………………………………………50 mg
*Cremophor® EL (polyoxyethylated castor oil)………………………………………………………..650 mg
alcohol, Ph. Helv. ……………………………………………………………………………32.9% by volume
nitrogen………………………………………………………………………………………………………….qs
which must be diluted further with 0.9% Sodium Chloride Injection or 5% Dextrose Injection using appropriate aseptic technique before use.
The chemical structure of cyclosporine (also known as cyclosporin A) is
HOW SUPPLIED SECTION
HOW SUPPLIED
Sandimmune**®**** Soft Gelatin Capsules (cyclosporine capsules, USP)**
25 mg: Oval, pink, branded “ 78/240”. Unit dose
packages of 30 capsules,
78/240”. Unit dose
packages of 30 capsules,
3 blister cards of 10 capsules………………………………………………………….NDC 0078-0240-15
100 mg: Oblong, dusty rose, branded “ 78/241”. Unit dose
packages of 30 capsules,
3 blister cards of 10 capsules………………………………………………………….NDC 0078-0241-15
Store and Dispense: Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C and 30°C (59°F and 86°F) [see USP Controlled Room Temperature].
An odor may be detected upon opening the unit dose container, which will dissipate shortly thereafter. This odor does not affect the quality of the product.
Sandimmune**®**** Oral Solution (cyclosporine oral solution, USP)**
Supplied in 50 mL bottles containing 100 mg of cyclosporine per mL NDC 0078-0110-22
A dosage syringe is provided for dispensing.
Store and Dispense: In the original container at temperatures below 30°C (86°F). Do not store in the refrigerator. Protect from freezing. Once opened, the contents must be used within 2 months.
Sandimmune**®**** Injection (cyclosporine injection, USP)**
FOR INTRAVENOUS INFUSION
Supplied as a 5 mL sterile ampul containing 50 mg of cyclosporine per mL,
in boxes of 10 ampuls…………………………………………………………………..NDC 0078-0109-01
Store and Dispense: At temperatures below 30°C (86°F). Protect from light.
FOR INFUSION ONLY
*Cremophor® is the registered trademark of BASF Aktiengesellschaft.
Distributed by:
Novartis Pharmaceuticals Corporation
East Hanover, New Jersey 07936
© Novartis
Revised: May 2025
T2025-29