
PANTOPRAZOLE SODIUM
These highlights do not include all the information needed to use PANTOPRAZOLE SODIUM DELAYED-RELEASE TABLETS safely and effectively. See full prescribing information for PANTOPRAZOLE SODIUM DELAYED-RELEASE TABLETS. PANTOPRAZOLE SODIUM delayed-release tablets, for oral use Initial U.S. approval: 2000
3540d01c-da0e-477e-9e90-994b96deb1d6
HUMAN PRESCRIPTION DRUG LABEL
Mar 13, 2024
Asclemed USA, Inc.
DUNS: 059888437
Products 2
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
PANTOPRAZOLE
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (17)
PANTOPRAZOLE
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (17)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
Pantoprazole sodium delayed-release tablets are indicated for:
1.1 Short-Term Treatment of Erosive Esophagitis Associated With
Gastroesophageal Reflux Disease (GERD)
Pantoprazole sodium delayed-release tablets are indicated in adults and pediatric patients five years of age and older for the short-term treatment (up to 8 weeks) in the healing and symptomatic relief of erosive esophagitis (EE). For those adult patients who have not healed after 8 weeks of treatment, an additional 8-week course of pantoprazole sodium delayed-release tablets may be considered. Safety of treatment beyond 8 weeks in pediatric patients has not been established.
1.2 Maintenance of Healing of Erosive Esophagitis
Pantoprazole sodium delayed-release tablets are indicated for maintenance of healing of EE and reduction in relapse rates of daytime and nighttime heartburn symptoms in adult patients with GERD. Controlled studies did not extend beyond 12 months.
1.3 Pathological Hypersecretory Conditions Including Zollinger-Ellison
Syndrome
Pantoprazole sodium delayed-release tablets are indicated for the long-term treatment of pathological hypersecretory conditions, including Zollinger- Ellison (ZE) Syndrome.
CONTRAINDICATIONS SECTION
4 CONTRAINDICATIONS
• Pantoprazole sodium delayed-release tablets are contraindicated in patients
with known hypersensitivity to any component of the formulation or any
substituted benzimidazole. Hypersensitivity reactions may include anaphylaxis,
anaphylactic shock, angioedema, bronchospasm, acute tubulointerstitial
nephritis, and urticaria [see Warnings and Precautions ( 5.2), Adverse Reactions ( 6)].
• Proton pump inhibitors (PPIs), including pantoprazole sodium delayed-release
tablets, are contraindicated in patients receiving rilpivirine-containing
products [see Drug Interactions ( 7)].
• Patients with known hypersensitivity to any component of the formulation or
to substituted benzimidazoles ( 4)
• Patients receiving rilpivirine-containing products ( 4, 7)
ADVERSE REACTIONS SECTION
6 ADVERSE REACTIONS
The following serious adverse reactions are described below and elsewhere in labeling:
• Acute Tubulointerstitial Nephritis [see Warnings and Precautions (5.2)]
• Clostridium difficile-Associated Diarrhea [see Warnings and Precautions (5.3)]
• Bone Fracture [see Warnings and Precautions (5.4)]
• Severe Cutaneous Adverse Reactions [seeWarnings and Precautions ( 5.5)]
• Cutaneous and Systemic Lupus Erythematosus [see Warningsand Precautions ( 5.6)]
• Cyanocobalamin (Vitamin B-12) Deficiency [see Warnings and Precautions ( 5.7)]
• Hypomagnesemia and Mineral Metabolism [see Warnings and Precautions ( 5.8)]
• Fundic Gland Polyps [see Warnings and Precautions (5.10)]
6.1 Clinical Trials Experience
The adverse reaction profiles for pantoprazole sodium for delayed-release oral suspension and pantoprazole sodium delayed-release tablets are similar.
Because clinical trials are conducted under widely varying conditions, adverse
reaction rates observed in the clinical trials of a drug cannot be directly
compared to rates in the clinical trials of another drug and may not reflect
the rates observed in clinical practice.
Adults
Safety in nine randomized comparative US clinical trials in patients with GERD
included 1,473 patients on oral pantoprazole sodium (20 mg or 40 mg), 299
patients on an H 2-receptor antagonist, 46 patients on another PPI, and 82
patients on placebo. The most frequently occurring adverse reactions are
listed in Table 3.
Table 3: Adverse Reactions Reported in Clinical Trials of Adult Patients
with GERD at a Frequency of >2%
|
Pantoprazole sodium |
Comparators |
Placebo | |
|
Headache |
12.2 |
12.8 |
8.5 |
|
Diarrhea |
8.8 |
9.6 |
4.9 |
|
Nausea |
7.0 |
5.2 |
9.8 |
|
Abdominal pain |
6.2 |
4.1 |
6.1 |
|
Vomiting |
4.3 |
3.5 |
2.4 |
|
Flatulence |
3.9 |
2.9 |
3.7 |
|
Dizziness |
3.0 |
2.9 |
1.2 |
|
Arthralgia |
2.8 |
1.4 |
1.2 |
Additional adverse reactions that were reported for pantoprazole sodium in
clinical trials with a frequency of ≤2% are listed below by body system:
Body as a Whole:allergic reaction, pyrexia, photosensitivity reaction, facial
edema
Gastrointestinal:constipation, dry mouth, hepatitis
Hematologic:leukopenia, thrombocytopenia
Metabolic/Nutritional:elevated CK (creatine kinase), generalized edema,
elevated triglycerides, liver enzymes elevated
Musculoskeletal:myalgia
Nervous:depression, vertigo
Skin and Appendages:urticaria, rash, pruritus
Special Senses:blurred vision
Pediatric Patients
Safety of pantoprazole sodium in the treatment of EE associated with GERD was
evaluated in pediatric patients ages 1 year through 16 years in three clinical
trials. Safety trials involved pediatric patients with EE; however, as EE is
uncommon in the pediatric population, 249 pediatric patients with
endoscopically-proven or symptomatic GERD were also evaluated. All adult
adverse reactions to pantoprazole sodium are considered relevant to pediatric
patients. In patients ages 1 year through 16 years, the most commonly reported
(>4%) adverse reactions include: URI, headache, fever, diarrhea, vomiting,
rash, and abdominal pain.
For safety information in patients less than 1 year of age see Use in Specific
Populations ( 8.4).
Additional adverse reactions that were reported for pantoprazole sodium in
pediatric patients in clinical trials with a frequency of ≤4% are listed below
by body system:
Body as a Whole:allergic reaction, facial edema
Gastrointestinal:constipation, flatulence, nausea
Metabolic/Nutritional:elevated triglycerides, elevated liver enzymes, elevated
CK (creatine kinase)
Musculoskeletal:arthralgia, myalgia
Nervous:dizziness, vertigo
Skin and Appendages:urticaria
The following adverse reactions seen in adults in clinical trials were not
reported in pediatric patients in clinical trials, but are considered relevant
to pediatric patients: photosensitivity reaction, dry mouth, hepatitis,
thrombocytopenia, generalized edema, depression, pruritus, leukopenia, and
blurred vision.
Zollinger-Ellison (ZE) Syndrome
In clinical studies of ZE Syndrome, adverse reactions reported in 35 patients
taking pantoprazole sodium 80 mg/day to 240 mg/day for up to 2 years were
similar to those reported in adult patients with GERD.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use
of pantoprazole sodium. Because these reactions are reported voluntarily from
a population of uncertain size, it is not always possible to reliably estimate
their frequency or establish a causal relationship to drug exposure.
These adverse reactions are listed below by body system:
Gastrointestinal Disorders:fundic gland polyps
General Disorders and Administration Conditions: asthenia, fatigue, malaise
Hematologic:pancytopenia, agranulocytosis
Hepatobiliary Disorders:hepatocellular damage leading to jaundice and hepatic
failure
Immune System Disorders:anaphylaxis (including anaphylactic shock), systemic
lupus erythematosus
Infections and Infestations:Clostridium difficile associated diarrhea
Investigations:weight changes
Metabolism and Nutritional Disorders:hypomagnesemia, hypocalcemia,
hypokalemia, hyponatremia
Musculoskeletal Disorders:rhabdomyolysis, bone fracture
Nervous:ageusia, dysgeusia
Psychiatric Disorders:hallucination, confusion, insomnia, somnolence
Renal and Genitourinary Disorders:acute tubulointerstitial nephritis, erectile
dysfunction
Skin and Subcutaneous Tissue Disorders: severe dermatologic reactions (some
fatal), including erythema multiforme, SJS/TEN, DRESS, AGEP, angioedema
(Quincke’s edema) and cutaneous lupus erythematosus
Most common adverse reactions are:
• For adult use (>2%): headache, diarrhea, nausea, abdominal pain, vomiting,
flatulence, dizziness, and arthralgia. ( 6.1)
• For pediatric use (>4%): URI, headache, fever, diarrhea, vomiting, rash, and
abdominal pain. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Hetero Labs Limited at
1-866-495-1995or FDA at 1-800-FDA-1088or
www.fda.gov/medwatch.
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
Table 4 includes drugs with clinically important drug interactions and interaction with diagnostics when administered concomitantly with pantoprazole sodium and instructions for preventing or managing them.
Consult the labeling of concomitantly used drugs to obtain further information about interactions with PPIs.
Table 4: Clinically Relevant Interactions Affecting Drugs Co-Administered with Pantoprazole Sodium and Interactions with Diagnostics
|
Antiretrovirals | |
|
Clinical Impact: |
The effect of PPIs on antiretroviral drugs is variable. The clinical
importance and the mechanisms behind these interactions are not always known. |
|
Intervention: |
Rilpivirine-containing products: Concomitant use with pantoprazole sodium is
contraindicated [see Contraindications ( 4)] . See prescribing information. |
|
Warfarin | |
|
Clinical Impact: |
Increased INR and prothrombin time in patients receiving PPIs, including pantoprazole, and warfarin concomitantly. Increases in INR and prothrombin time may lead to abnormal bleeding and even death. |
|
Intervention: |
Monitor INR and prothrombin time. Dose adjustment of warfarin may be needed to maintain target INR range. See prescribing information for warfarin. |
|
Clopidogrel | |
|
Clinical Impact: |
Concomitant administration of pantoprazole and clopidogrel in healthy subjects had no clinically important effect on exposure to the active metabolite of clopidogrel or clopidogrel-induced platelet inhibition [see Clinical Pharmacology ( 12.3)]. |
|
Intervention: |
No dose adjustment of clopidogrel is necessary when administered with an approved dose of pantoprazole sodium. |
|
Methotrexate | |
|
Clinical Impact: |
Concomitant use of PPIs with methotrexate (primarily at high dose) may elevate and prolong serum concentrations of methotrexate and/or its metabolite hydroxymethotrexate, possibly leading to methotrexate toxicities. No formal drug interaction studies of high-dose methotrexate with PPIs have been conducted [see Warnings and Precautions ( 5.13)] . |
|
Intervention: |
A temporary withdrawal of pantoprazole sodium may be considered in some patients receiving high-dose methotrexate. |
|
Drugs Dependent on Gastric pH for Absorption (e.g., iron salts, erlotinib, dasatinib, nilotinib, mycophenolate mofetil, ketoconazole**/itraconazole)** | |
|
Clinical Impact: |
Pantoprazole can reduce the absorption of other drugs due to its effect on reducing intragastric acidity. |
|
Intervention: |
Mycophenolate mofetil (MMF): Co-administration of pantoprazole sodium in
healthy subjects and in transplant patients receiving MMF has been reported to
reduce the exposure to the active metabolite, mycophenolic acid (MPA),
possibly due to a decrease in MMF solubility at an increased gastric pH [see Clinical Pharmacology ( 12.3)] . The clinical relevance of reduced MPA
exposure on organ rejection has not been established in transplant patients
receiving pantoprazole sodium and MMF. Use pantoprazole sodium with caution in
transplant patients receiving MMF. |
|
Interactions with Investigations of Neuroendocrine Tumors | |
|
Clinical Impact: |
CgA levels increase secondary to PPI-induced decreases in gastric acidity. The increased CgA level may cause false positive results in diagnostic investigations for neuroendocrine tumors [see Warnings and Precautions (5.11), Clinical Pharmacology ( 12.2)] . |
|
Intervention: |
Temporarily stop pantoprazole sodium treatment at least 14 days before assessing CgA levels and consider repeating the test if initial CgA levels are high. If serial tests are performed (e.g., for monitoring), the same commercial laboratory should be used for testing, as reference ranges between tests may vary. |
|
False Positive Urine Tests for THC | |
|
Clinical Impact: |
There have been reports of false positive urine screening tests for tetrahydrocannabinol (THC) in patients receiving PPIs [see Warnings and Precautions ( 5.12)] . |
|
Intervention: |
An alternative confirmatory method should be considered to verify positive results. |
See full prescribing information for a list of clinically important drug interactions (7)
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosing Schedule
Pantoprazole sodium is supplied as delayed-release tablets. The recommended
dosages are outlined in Table 1.
Table 1: Recommended Dosing Schedule for
** Pantoprazole Sodium Delayed-Release Tablets**
|
Indication |
Dose |
Frequency |
|
Short-Term Treatment of Erosive Esophagitis Associated With GERD | ||
|
Adults |
40 mg |
Once daily for up to 8 weeks* |
|
Children (5 years and older) |
20 mg |
Once daily for up to 8 weeks |
|
≥ 40 kg |
40 mg | |
|
** Maintenance of Healing of Erosive Esophagitis** | ||
|
Adults |
40 mg |
Once daily*** |
|
Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome | ||
|
Adults |
40 mg |
Twice daily** |
- For adult patients who have not healed after 8 weeks of treatment, an additional 8-week course of pantoprazole sodium delayed-release tablets may be considered.
** Dosage regimens should be adjusted to individual patient needs and should continue for as long as clinically indicated. Doses up to 240 mg daily have been administered.
*** Controlled studies did not extend beyond 12 months
2.2 Administration Instructions
Directions for method of administration for each dosage form are presented in
Table 2.
** Tab****le 2: Administration Instructions**
|
Formulation |
Route |
Instructions* | |
|
Delayed-Release Tablets |
Oral |
Swallowed whole, with or without food |
- Do not split, chew, or crush pantoprazole sodium delayed-release tablets.
Take a missed dose as soon as possible. If it is almost time for the next dose, skip the missed dose and take the next dose at the regular scheduled time. Do not take 2 doses at the same time.
Pantoprazole Sodium Delayed-Release Tablets
Swallow pantoprazole sodium delayed-release tablets whole, with or without food in the stomach. For patients unable to swallow a 40 mg tablet, two 20 mg tablets may be taken. Concomitant administration of antacids does not affect the absorption of pantoprazole sodium delayed-release tablets.
|
Indication |
Dose |
Frequency |
|
Short-Term Treatment of Erosive Esophagitis Associated With GERD ( 2.1) | ||
|
Adults |
40 mg |
Once Daily for up to 8 wks |
|
Children (5 years and | ||
|
≥ 15 kg to < 40 kg |
20 mg |
Once Daily for up to 8 wks |
|
≥ 40 kg |
40 mg | |
|
Maintenance of Healing of Erosive Esophagitis (2.1) | ||
|
Adults |
40 mg |
Once Daily* |
|
Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome (2.1) | ||
|
Adults |
40 mg |
Twice Daily |
- Controlled studies did not extend beyond 12 months
See full prescribing information for administration instructions
DOSAGE FORMS & STRENGTHS SECTION
3 DOSAGE FORMS AND STRENGTHS
• 20 mg, yellow to pale yellow, oval, biconvex, delayed-release tablets imprinted “H125” on one side with black ink and plain on the other side.
• 40 mg, yellow to pale yellow, oval, biconvex, delayed-release tablets imprinted “H126” on one side with black ink and plain on the other side.
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Available data from published observational studies did not demonstrate an
association of major malformations or other adverse pregnancy outcomes with
pantoprazole.
In animal reproduction studies, no evidence of adverse development outcomes
was observed with pantoprazole. Reproduction studies have been performed in
rats at oral doses up to 450 mg/kg/day (about 88 times the recommended human
dose) and rabbits at oral doses up to 40 mg/kg/day (about 16 times the
recommended human dose) with administration of pantoprazole during
organogenesis in pregnant animals and have revealed no evidence of harm to the
fetus due to pantoprazole in this study (see Data).
A pre-and postnatal development toxicity study in rats with additional
endpoints to evaluate the effect on bone development was performed with
pantoprazole sodium. Oral pantoprazole doses of 5, 15, and 30 mg/kg/day
(approximately 1, 3, and 6 times the human dose of 40 mg/day) were
administered to pregnant females from gestation day (GD) 6 through lactation
day (LD) 21. Changes in bone morphology were observed in pups exposed to
pantoprazole in uteroand through milk during the period of lactation as well
as by oral dosing from postnatal day (PND) 4 through PND 21 [see Use in Specific Populations ( 8.4)]. There were no drug-related findings in maternal
animals. Advise pregnant women of the potential risk of fetal harm.
The estimated background risk of major birth defects and miscarriage for the
indicated population is unknown. All pregnancies have a background risk of
birth defect, loss or other adverse outcomes. In the U.S. general population,
the estimated background risk of major birth defects and miscarriage in the
clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Data
Human Data
Available data from published observational studies failed to demonstrate an
association of adverse pregnancy-related outcomes and pantoprazole use.
Methodological limitations of these observational studies cannot definitely
establish or exclude any drug-associated risk during pregnancy. In a
prospective study by the European Network of Teratology Information Services,
outcomes from a group of 53 pregnant women administered median daily doses of
40 mg pantoprazole were compared to a control group of 868 pregnant women who
did not take any proton pump inhibitors (PPIs). There was no difference in the
rate of major malformations between women exposed to PPIs and the control
group, corresponding to a Relative Risk (RR)=0.55, [95% Confidence Interval (CI) 0.08-3.95]. In a population-based retrospective cohort study covering all
live births in Denmark from 1996 to 2008, there was no significant increase in
major birth defects during analysis of first trimester exposure to
pantoprazole in 549 live births. A meta-analysis that compared 1,530 pregnant
women exposed to PPIs in at least the first trimester with 133,410 unexposed
pregnant women showed no significant increases in risk for congenital
malformations or spontaneous abortion with exposure to PPIs (for major
malformations OR=1.12 ([95% CI 0.86-1.45] and for spontaneous abortions
OR=1.29 [95% CI 0.84-1.97]).
Animal Data
Reproduction studies have been performed in rats at oral pantoprazole doses up
to 450 mg/kg/day (about 88 times the recommended human dose based on body
surface area) and in rabbits at oral doses up to 40 mg/kg/day (about 16 times
the recommended human dose based on body surface area) with administration of
pantoprazole sodium during organogenesis in pregnant animals. The studies have
revealed no evidence of impaired fertility or harm to the fetus due to
pantoprazole.
A pre- and postnatal development toxicity study in rats with additional
endpoints to evaluate the effect on bone development was performed with
pantoprazole sodium. Oral pantoprazole doses of 5, 15, and 30 mg/kg/day
(approximately 1, 3, and 6 times the human dose of 40 mg/day on a body surface
area basis) were administered to pregnant females from gestation day (GD) 6
through lactation day (LD) 21. On postnatal day (PND 4) through PND 21, the
pups were administered oral doses at 5, 15, and 30 mg/kg/day (approximately 1,
2.3, and 3.2 times the exposure (AUC) in humans at a dose of 40 mg). There
were no drug-related findings in maternal animals. During the preweaning
dosing phase (PND 4 to 21) of the pups, there were increased mortality and/or
moribundity and decreased body weight and body weight gain at 5 mg/kg/day
(approximately equal exposures (AUC) in humans receiving the 40 mg dose) and
higher doses. On PND 21, decreased mean femur length and weight and changes in
femur bone mass and geometry were observed in the offspring at 5 mg/kg/day
(approximately equal exposures (AUC) in humans at the 40 mg dose) and higher
doses. The femur findings included lower total area, bone mineral content and
density, periosteal and endosteal circumference, and cross-sectional moment of
inertia. There were no microscopic changes in the distal femur, proximal
tibia, or stifle joints. Changes in bone parameters were partially reversible
following a recovery period, with findings on PND 70 limited to lower femur
metaphysis cortical/subcortical bone mineral density in female pups at 5
mg/kg/day (approximately equal exposures (AUC) in humans at the 40 mg dose)
and higher doses.
8.2 Lactation
Risk Summary
Pantoprazole has been detected in breast milk of a nursing mother after a
single 40 mg oral dose of pantoprazole. There were no effects on the breastfed
infant (see Data).There are no data on pantoprazole effects on milk
production.
The developmental and health benefits of breastfeeding should be considered
along with the mother’s clinical need for pantoprazole sodium and any
potential adverse effects on the breastfed child from pantoprazole or from the
underlying maternal condition.
Data
The breast milk of a 42-year-old woman receiving 40 mg of oral pantoprazole,
at 10 months postpartum, was studied for 24 hours, to demonstrate low levels
of pantoprazole present in the breast milk. Pantoprazole was detectable in
milk only 2 and 4 hours after the dose with milk levels of approximately 36
mcg/L and 24 mcg/L, respectively. A milk-to-plasma ratio of 0.022 was observed
at 2 hours after drug administration. Pantoprazole was not detectable (<10
mcg/L) in milk at 6, 8 and 24 hours after the dose. The relative dose to the
infant was estimated to be 7.3 mcg of pantoprazole, which is equivalent to
0.14% of the weight-adjusted maternal dose. No adverse events in the infant
were reported by the mother.
8.4 Pediatric Use
The safety and effectiveness of pantoprazole sodium for short-term treatment
(up to eight weeks) of EE associated with GERD have been established in
pediatric patients 1 year through 16 years of age. Effectiveness for EE has
not been demonstrated in patients less than 1 year of age. In addition, for
patients less than 5 years of age, there is no appropriate dosage strength in
an age-appropriate formulation available. Therefore, pantoprazole sodium is
indicated for the short-term treatment of EE associated with GERD for patients
5 years and older. The safety and effectiveness of pantoprazole sodium for
pediatric uses other than EE have not been established.
1 year through 16 years of age
Use of pantoprazole sodium in pediatric patients 1 year through 16 years of
age for short-term treatment (up to eight weeks) of EE associated with GERD is
supported by: a) extrapolation of results from adequate and well-controlled
studies that supported the approval of pantoprazole sodium for treatment of EE
associated with GERD in adults, and b) safety, effectiveness, and
pharmacokinetic studies performed in pediatric patients [see Clinical Studies ( 14.1), Clinical Pharmacology ( 12.3)].
Safety of pantoprazole sodium in the treatment of EE associated with GERD in
pediatric patients 1 through 16 years of age was evaluated in three
multicenter, randomized, double-blind, parallel- treatment studies, involving
249 pediatric patients, including 8 with EE (4 patients ages 1 year to 5 years
and 4 patients 5 years to 11 years). The children ages 1 year to 5 years with
endoscopically diagnosed EE (defined as an endoscopic Hetzel-Dent score ≥ 2)
were treated once daily for 8 weeks with one of two dose levels of
pantoprazole sodium (approximating 0.6 mg/kg or 1.2 mg/kg). All 4 of these
patients with EE were healed (Hetzel-Dent score of 0 or 1) at 8 weeks. Because
EE is uncommon in the pediatric population, predominantly pediatric patients
with endoscopically-proven or symptomatic GERD were also included in these
studies. Patients were treated with a range of doses of pantoprazole sodium
once daily for 8 weeks. For safety findings see Adverse Reactions ( 6.1).
Because these pediatric trials had no placebo, active comparator, or evidence
of a dose response, the trials were inconclusive regarding the clinical
benefit of pantoprazole sodium for symptomatic GERD in the pediatric
population. The effectiveness of pantoprazole sodium for treating symptomatic
GERD in pediatric patients has not been established.
Although the data from the clinical trials support use of pantoprazole sodium
for the short-term treatment of EE associated with GERD in pediatric patients
1 year through 5 years, there is no commercially available dosage formulation
appropriate for patients less than 5 years of age [see Dosage and Administration ( 2)].
In a population pharmacokinetic analysis, clearance values in the children 1
to 5 years old with endoscopically proven GERD had a median value of 2.4 L/h.
Following a 1.2 mg/kg equivalent dose (15 mg for ≤12.5 kg and 20 mg for >12.5
to <25 kg), the plasma concentrations of pantoprazole were highly variable and
the median time to peak plasma concentration was 3 to 6 hours. The estimated
AUC for patients 1 to 5 years old was 37% higher than for adults receiving a
single 40 mg tablet, with a geometric mean AUC value of 6.8 mcg•hr/mL.
Neonates to less than one year of age
Pantoprazole sodium was not found to be effective in a multicenter,
randomized, double-blind, placebo-controlled, treatment-withdrawal study of
129 pediatric patients 1 through 11 months of age. Patients were enrolled if
they had symptomatic GERD based on medical history and had not responded to
non-pharmacologic interventions for GERD for two weeks. Patients received
pantoprazole sodium daily for four weeks in an open-label phase, then patients
were randomized in equal proportion to receive pantoprazole sodium treatment
or placebo for the subsequent four weeks in a double-blind manner. Efficacy
was assessed by observing the time from randomization to study discontinuation
due to symptom worsening during the four-week treatment-withdrawal phase.
There was no statistically significant difference between pantoprazole sodium
and placebo in the rate of discontinuation.
In this trial, the adverse reactions that were reported more commonly
(difference of ≥4%) in the treated population compared to the placebo
population were elevated CK, otitis media, rhinitis, and laryngitis.
In a population pharmacokinetic analysis, the systemic exposure was higher in
patients less than 1 year of age with GERD compared to adults who received a
single 40 mg dose (geometric mean AUC was 103% higher in preterm infants and
neonates receiving single dose of 2.5 mg of pantoprazole sodium, and 23%
higher in infants 1 through 11 months of age receiving a single dose of
approximately 1.2 mg/kg). In these patients, the apparent clearance (CL/F)
increased with age (median clearance: 0.6 L/hr, range: 0.03 to 3.2 L/hr).
These doses resulted in pharmacodynamic effects on gastric but not esophageal
pH. Following once daily dosing of 2.5 mg of pantoprazole sodium in preterm
infants and neonates, there was an increase in the mean gastric pH (from 4.3
at baseline to 5.2 at steady-state) and in the mean % time that gastric pH was
4 (from 60% at baseline to 80% at steady-state). Following once daily dosing of approximately 1.2 mg/kg of pantoprazole sodium in infants 1 through 11 months of age, there was an increase in the mean gastric pH (from 3.1 at baseline to 4.2 at steady-state) and in the mean % time that gastric pH was > 4 (from 32% at baseline to 60% at steady-state). However, no significant changes were observed in mean intraesophageal pH or % time that esophageal pH was <4 in either age group.
Because pantoprazole sodium was not shown to be effective in the randomized, placebo-controlled study in this age group, the use of pantoprazole sodium for treatment of symptomatic GERD in infants less than 1 year of age is not indicated.
Animal Toxicity Data
In a pre- and post-natal development study in rats, the pups were administered oral doses of pantoprazole at 5, 15, and 30 mg/kg/day (approximately 1, 2.3, and 3.2 times the exposure(AUC) in children aged 6 to 11 years at a dose of 40 mg) on postnatal day (PND 4) through PND 21, in addition to lactational exposure through milk. On PND 21, decreased mean femur length and weight and changes in femur bone mass and geometry were observed in the offspring at 5 mg/kg/day (approximately equal exposures (AUC) in children aged 6 to 11 years at the 40 mg dose) and higher doses. Changes in bone parameters were partially reversible following a recovery period.
In neonatal/juvenile animals (rats and dogs) toxicities were similar to those observed in adult animals, including gastric alterations, decreases in red cell mass, increases in lipids, enzyme induction and hepatocellular hypertrophy. An increased incidence of eosinophilic chief cells in adult and neonatal/juvenile rats, and atrophy of chief cells in adult rats and in neonatal/juvenile dogs, was observed in the fundic mucosa of stomachs in repeated-dose studies. Full to partial recovery of these effects were noted in animals of both age groups following a recovery period.
8.5 Geriatric Use
In short-term US clinical trials, EE healing rates in the 107 elderly patients (≥65 years old) treated with pantoprazole sodium were similar to those found in patients under the age of 65. The incidence rates of adverse reactions and laboratory abnormalities in patients aged 65 years and older were similar to those associated with patients younger than 65 years of age.
Pregnancy: Based on animal data, may cause fetal harm. ( 8.1)
OVERDOSAGE SECTION
10 OVERDOSAGE
Experience in patients taking very high doses of pantoprazole sodium (greater
than 240 mg) is limited. Spontaneous post-marketing reports of overdose are
generally within the known safety profile of pantoprazole sodium.
Pantoprazole is not removed by hemodialysis. In case of overdosage, treatment
should be symptomatic and supportive.
Single oral doses of pantoprazole at 709 mg/kg, 798 mg/kg, and 887 mg/kg were
lethal to mice, rats, and dogs, respectively. The symptoms of acute toxicity
were hypoactivity, ataxia, hunched sitting, limb-splay, lateral position,
segregation, absence of ear reflex, and tremor.
If overexposure to pantoprazole sodium occurs, call your Poison Control Center
at 1-800-222-1222 for current information on the management of poisoning or
overdosage.
DESCRIPTION SECTION
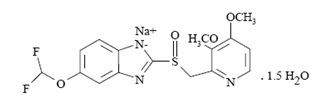
11 DESCRIPTION
The active ingredient in pantoprazole sodium delayed-release tablets, USP, a PPI, is a substituted benzimidazole, 5-(Difluoromethoxy)-2-[[(3,4-dimethoxy-2-pyridyl)methyl] sulfinyl]benzimidazole, sodium salt, sesquihydrate, a compound that inhibits gastric acid secretion. Its empirical formula is C 16H 14F 2N 3NaO 4S . 1.5 H 2O, with a molecular weight of 432.4. The structural formula is:
Pantoprazole sodium sesquihydrate, USP is a white to off-white powder.
Pantoprazole sodium sesquihydrate, USP is freely soluble in water, in
methanol, in dehydrated alcohol, practically insoluble in hexane and
dichloromethane.
The stability of the compound in aqueous solution is pH-dependent. The rate of
degradation increases with decreasing pH. At ambient temperature, the
degradation half-life is approximately 2.8 hours at pH 5 and approximately 220
hours at pH 7.8.
Pantoprazole Sodium is supplied as a delayed-release tablet, available in two
strengths (20 mg and 40 mg).
Each Pantoprazole Sodium Delayed-Release Tablet, USP contains 45.11 mg or
22.55 mg of pantoprazole sodium sesquihydrate, USP (equivalent to 40 mg or 20
mg pantoprazole, respectively) with the following inactive ingredients:
calcium stearate, carnauba wax, ferric oxide yellow, hydroxy propyl cellulose,
hypromellose, lactose monohydrate, methacrylic acid copolymer, polysorbate 80,
propylene glycol, sodium carbonate anhydrous, sodium lauryl sulfate, titanium
dioxide and triethyl citrate. The tablets are imprinted with opacode black
containing ammonium hydroxide, iron oxide black, propylene glycol and shellac.
Pantoprazole Sodium Delayed-Release Tablets, (40 mg and 20 mg) complies with
USP dissolution test 2.
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
Pantoprazole Sodium Delayed-Release Tablets, USP are supplied as 20 mg yellow to pale yellow, oval, biconvex, delayed-release tablets imprinted “H125” on one side with black ink and plain on the other side. They are supplied as follows:
Bottles of 10 tablets NDC 76420-671-10 (repackaged from 31722-712-XX)
Bottles of 30 tablets NDC 76420-671-30 (repackaged from 31722-712-XX)
Bottles of 60 tablets NDC 76420-671-60 (repackaged from 31722-712-XX)
Bottles of 90 tablets NDC 76420-671-90 (relabeled from 31722-712-90)
Bottles of 100 tablets NDC 76420-671-01 (repackaged from 31722-712-XX)
Pantoprazole Sodium Delayed-Release Tablets, USP are supplied as 40 mg yellow to pale yellow, oval, biconvex, delayed-release tablets imprinted “H126” on one side with black ink and plain on the other side. They are supplied as follows:
Bottles of 10 tablets NDC 76420-674-10 (repackaged from 31722-713-XX)
Bottles of 30 tablets NDC 76420-674-30 (repackaged from 31722-713-XX)
Bottles of 60 tablets NDC 76420-674-60 (repackaged from 31722-713-XX)
Bottles of 90 tablets NDC 76420-674-90 (relabeled and repackaged from 31722-713-90)
Bottles of 100 tablets NDC 76420-674-01 (repackaged from 31722-713-XX)
Storage
Store pantoprazole sodium delayed-release tablets, USP at 20° to 25°C (68° to
77°F) [see USP Controlled Room Temperature].
SPL MEDGUIDE SECTION
MEDICATION GUIDE
|
Pantoprazole Sodium Delayed-Release Tablets USP |
|
What is the most important information I should know about pantoprazole
sodium delayed-release tablets? |
|
What are pantoprazole sodium delayed-release tablets? |
|
Do not take pantoprazole sodium delayed-release tablets if you are: |
|
Before taking pantoprazole sodium delayed-release tablets, tell your doctor
about all of your medical conditions, including if you:**** |
|
How should I take pantoprazole sodium delayed-release tablets? |
|
What are the possible side effects of pantoprazole sodium delayed-release
tablets? |
|
How should I store pantoprazole sodium delayed-release tablets? |
|
What are the ingredients in pantoprazole sodium delayed-release tablets? |
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Relabeled and Repackaged by:
Enovachem PHARMACEUTICALS
Torrance, CA 90501
CLINICAL PHARMACOLOGY SECTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Pantoprazole is a PPI that suppresses the final step in gastric acid production by covalently binding to the (H +, K +)-ATPase enzyme system at the secretory surface of the gastric parietal cell. This effect leads to inhibition of both basal and stimulated gastric acid secretion, irrespective of the stimulus. The binding to the (H +, K +)-ATPase results in a duration of antisecretory effect that persists longer than 24 hours for all doses tested (20 mg to 120 mg).
12.2 Pharmacodynamics
Antisecretory Activity
Under maximal acid stimulatory conditions using pentagastrin, a dose-dependent
decrease in gastric acid output occurs after a single dose of oral (20 to 80
mg) or a single dose of intravenous (20 to 120 mg) pantoprazole in healthy
subjects. Pantoprazole given once daily results in increasing inhibition of
gastric acid secretion. Following the initial oral dose of 40 mg pantoprazole,
a 51% mean inhibition was achieved by 2.5 hours. With once-a-day dosing for 7
days, the mean inhibition was increased to 85%. Pantoprazole suppressed acid
secretion in excess of 95% in half of the subjects. Acid secretion had
returned to normal within a week after the last dose of pantoprazole; there
was no evidence of rebound hypersecretion.
In a series of dose-response studies, pantoprazole, at oral doses ranging from
20 to 120 mg, caused dose-related increases in median basal gastric pH and in
the percent of time gastric pH was >3 and >4. Treatment with 40 mg of
pantoprazole produced significantly greater increases in gastric pH than the
20 mg dose. Doses higher than 40 mg (60, 80, 120 mg) did not result in further
significant increases in median gastric pH. The effects of pantoprazole on
median pH from one double-blind crossover study are shown in Table 5.
Table 5: Effect of Single Daily Doses of Oral Pantoprazole on Intragastric pH
|
———————Median pH on day 7——————— | ||||
|
Time |
Placebo |
20 mg |
40 mg |
80 mg |
|
8 a.m. - 8 a.m. |
1.3 |
2.9* |
3.8*# |
3.9*# |
|
8 a.m. - 10 p.m. |
1.6 |
3.2* |
4.4*# |
4.8*# |
|
10 p.m. - 8 a.m. |
1.2 |
2.1* |
3.0* |
2.6* |
*Significantly different from placebo
#Significantly different from 20 mg
Serum Gastrin Effects
Fasting serum gastrin levels were assessed in two double-blind studies of the
acute healing of EE in which 682 patients with gastroesophageal reflux disease
(GERD) received 10, 20, or 40 mg of pantoprazole sodium for up to 8 weeks. At
4 weeks of treatment there was an increase in mean gastrin levels of 7%, 35%,
and 72% over pretreatment values in the 10, 20, and 40 mg treatment groups,
respectively. A similar increase in serum gastrin levels was noted at the
8-week visit with mean increases of 3%, 26%, and 84% for the three
pantoprazole dose groups. Median serum gastrin levels remained within normal
limits during maintenance therapy with pantoprazole sodium delayed-release
tablets.
In long-term international studies involving over 800 patients, a 2- to 3-fold
mean increase from the pretreatment fasting serum gastrin level was observed
in the initial months of treatment with pantoprazole at doses of 40 mg per day
during GERD maintenance studies and 40 mg or higher per day in patients with
refractory GERD. Fasting serum gastrin levels generally remained at
approximately 2 to 3 times baseline for up to 4 years of periodic follow-up in
clinical trials.
Following short-term treatment with pantoprazole sodium, elevated gastrin
levels return to normal by at least 3 months.
Enterochromaffin-Like (ECL) Cell Effects
In 39 patients treated with oral pantoprazole 40 mg to 240 mg daily (majority
receiving 40 mg to 80 mg) for up to 5 years, there was a moderate increase in
ECL-cell density, starting after the first year of use, which appeared to
plateau after 4 years.
In a nonclinical study in Sprague-Dawley rats, lifetime exposure (24 months)
to pantoprazole at doses of 0.5 to 200 mg/kg/day resulted in dose-related
increases in gastric ECL-cell proliferation and gastric neuroendocrine
(NE)-cell tumors. Gastric NE-cell tumors in rats may result from chronic
elevation of serum gastrin concentrations. The high density of ECL cells in
the rat stomach makes this species highly susceptible to the proliferative
effects of elevated gastrin concentrations produced by PPIs. However, there
were no observed elevations in serum gastrin following the administration of
pantoprazole at a dose of 0.5 mg/kg/day. In a separate study, a gastric NE-
cell tumor without concomitant ECL-cell proliferative changes was observed in
1 female rat following 12 months of dosing with pantoprazole at 5 mg/kg/day
and a 9 month off-dose recovery [see Nonclinical Toxicology ( 13.1)].
Endocrine Effects
In a clinical pharmacology study, pantoprazole sodium 40 mg given once daily
for 2 weeks had no effect on the levels of the following hormones: cortisol,
testosterone, triiodothyronine (T 3), thyroxine (T 4), thyroid-stimulating
hormone (TSH), thyronine-binding protein, parathyroid hormone, insulin,
glucagon, renin, aldosterone, follicle-stimulating hormone, luteinizing
hormone, prolactin, and growth hormone.
In a 1-year study of GERD patients treated with pantoprazole sodium 40 mg or
20 mg, there were no changes from baseline in overall levels of T 3, T 4, and
TSH.
12.3 Pharmacokinetics
Pantoprazole sodium delayed-release tablets are prepared as enteric-coated
tablets so that absorption of pantoprazole begins only after the tablet leaves
the stomach. Peak serum concentration (C max) and area under the serum
concentration time curve (AUC) increase in a manner proportional to oral and
intravenous doses from 10 mg to 80 mg. Pantoprazole does not accumulate, and
its pharmacokinetics are unaltered with multiple daily dosing. Following oral
or intravenous administration, the serum concentration of pantoprazole
declines biexponentially, with a terminal elimination half-life of
approximately one hour.
In extensive metabolizers with normal liver function receiving an oral dose of
the enteric-coated 40 mg pantoprazole tablet, the peak concentration (C max)
is 2.5 mcg/mL; the time to reach the peak concentration (t max) is 2.5 h, and
the mean total area under the plasma concentration versus time curve (AUC) is
4.8 mcg•h/mL (range 1.4 to 13.3 mcg•h/mL). Following intravenous
administration of pantoprazole to extensive metabolizers, its total clearance
is 7.6 to 14.0 L/h, and its apparent volume of distribution is 11.0 to 23.6 L.
Absorption
After administration of a single or multiple oral 40 mg doses of pantoprazole
sodium delayed-release tablets, the peak plasma concentration of pantoprazole
was achieved in approximately 2.5 hours, and C maxwas 2.5 mcg/mL. Pantoprazole
undergoes little first-pass metabolism, resulting in an absolute
bioavailability of approximately 77%. Pantoprazole absorption is not affected
by concomitant administration of antacids.
Administration of pantoprazole sodium delayed-release tablets with food may
delay its absorption up to 2 hours or longer; however, the C maxand the extent
of pantoprazole absorption (AUC) are not altered. Thus, pantoprazole sodium
delayed-release tablets may be taken without regard to timing of meals.
Distribution
The apparent volume of distribution of pantoprazole is approximately 11 to
23.6 L, distributing mainly in extracellular fluid. The serum protein binding
of pantoprazole is about 98%, primarily to albumin.
Elimination
Metabolism
Pantoprazole is extensively metabolized in the liver through the cytochrome
P450 (CYP) system. Pantoprazole metabolism is independent of the route of
administration (intravenous or oral). The main metabolic pathway is
demethylation, by CYP2C19, with subsequent sulfation; other metabolic pathways
include oxidation by CYP3A4. There is no evidence that any of the pantoprazole
metabolites have significant pharmacologic activity.
Excretion
After a single oral or intravenous dose of 14C-labeled pantoprazole to
healthy, normal metabolizer subjects, approximately 71% of the dose was
excreted in the urine, with 18% excreted in the feces through biliary
excretion. There was no renal excretion of unchanged pantoprazole.
Specific Populations
Geriatric Patients
Only slight to moderate increases in the AUC (43%) and C max(26%) of
pantoprazole were found in elderly subjects (64 to 76 years of age) after
repeated oral administration, compared with younger subjects [see Use in Specific Populations ( 8.5)].
Pediatric Patients
The pharmacokinetics of pantoprazole were studied in children less than 16
years of age in four randomized, open-label clinical trials in pediatric
patients with presumed/proven GERD. Pantoprazole sodium delayed-release
tablets were studied in children older than 5 years.
In a population PK analysis, total clearance increased with increasing
bodyweight in a non-linear fashion. The total clearance also increased with
increasing age only in children under 3 years of age.
Neonate through 5 Years of Age[see Use in Specific Populations ( 8.4)]
Children and Adolescents 6 through 16 Years of Age
The pharmacokinetics of pantoprazole sodium delayed-release tablets were
evaluated in children ages 6 through 16 years with a clinical diagnosis of
GERD. The PK parameters following a single oral dose of 20 mg or 40 mg of
pantoprazole sodium delayed-release tablets in children ages 6 through 16
years were highly variable (%CV ranges 40 to 80%). The geometric mean AUC
estimated from population PK analysis after a 40 mg pantoprazole sodium
delayed-release tablet in pediatric patients was about 39% and 10% higher
respectively in 6 to 11 and 12 to 16 year-old children, compared to that of
adults (Table 7).
Table 7: PK Parameters in Children and Adolescents 6 through 16 years with GERD receiving 40 mg Pantoprazole Sodium Delayed-Release Tablets
|
6 to 11 years (n=12) |
12 to 16 years (n=11) | |
|
C max(mcg/mL) a |
1.8 |
1.8 |
aGeometric mean values
bMedian values
Male and Female Patients
There is a modest increase in pantoprazole AUC and C maxin women compared to
men. However, weight-normalized clearance values are similar in women and men.
In pediatric patients ages 1 through 16 years there were no clinically
relevant effects of gender on clearance of pantoprazole, as shown by
population pharmacokinetic analysis.
Patients with Renal Impairment
In patients with severe renal impairment, pharmacokinetic parameters for
pantoprazole were similar to those of healthy subjects.
Patients with Hepatic Impairment
In patients with mild to severe hepatic impairment (Child-Pugh A to C
cirrhosis), maximum pantoprazole concentrations increased only slightly
(1.5-fold) relative to healthy subjects. Although serum half-life values
increased to 7 to 9 hours and AUC values increased by 5- to 7-fold in hepatic-
impaired patients, these increases were no greater than those observed in
CYP2C19 poor metabolizers, where no dosage adjustment is warranted. These
pharmacokinetic changes in hepatic-impaired patients result in minimal drug
accumulation following once-daily, multiple-dose administration. Doses higher
than 40 mg/day have not been studied in hepatically impaired patients.
Drug Interaction Studies
Effect of Other Drugs on Pantoprazole
Pantoprazole is metabolized mainly by CYP2C19 and to minor extents by CYPs
3A4, 2D6, and 2C9. In in vivodrug-drug interaction studies with CYP2C19
substrates (diazepam [also a CYP3A4 substrate] and phenytoin [also a CYP3A4 inducer] and clopidogrel), nifedipine, midazolam, and clarithromycin (CYP3A4
substrates), metoprolol (a CYP2D6 substrate), diclofenac, naproxen and
piroxicam (CYP2C9 substrates), and theophylline (a CYP1A2 substrate) in
healthy subjects, the pharmacokinetics of pantoprazole were not significantly
altered.
Effect of Pantoprazole on Other Drugs
Clopidogrel
Clopidogrel is metabolized to its active metabolite in part by CYP2C19. In a
crossover clinical study, 66 healthy subjects were administered clopidogrel
(300 mg loading dose followed by 75 mg per day) alone and with pantoprazole
(80 mg at the same time as clopidogrel) for 5 days. On Day 5, the mean AUC of
the active metabolite of clopidogrel was reduced by approximately 14%
(geometric mean ratio was 86%, with 90% CI of 79 to 93%) when pantoprazole was
coadministered with clopidogrel as compared to clopidogrel administered alone.
Pharmacodynamic parameters were also measured and demonstrated that the change
in inhibition of platelet aggregation (induced by 5 µM ADP) was correlated
with the change in the exposure to clopidogrel active metabolite. The clinical
significance of this finding is not clear.
Mycophenolate Mofetil (MMF)
Administration of pantoprazole 40 mg twice daily for 4 days and a single 1000
mg dose of MMF approximately one hour after the last dose of pantoprazole to
12 healthy subjects in a cross-over study resulted in a 57% reduction in the C
maxand 27% reduction in the AUC of MPA. Transplant patients receiving
approximately 2000 mg per day of MMF (n=12) were compared to transplant
patients receiving approximately the same dose of MMF and pantoprazole 40 mg
per day (n=21). There was a 78% reduction in the C maxand a 45% reduction in
the AUC of MPA in patients receiving both pantoprazole and MMF [see Drug Interactions ( 7)].
Other Drugs
In vivostudies also suggest that pantoprazole does not significantly affect
the kinetics of the following drugs (cisapride, theophylline, diazepam [and its active metabolite, desmethyldiazepam], phenytoin, metoprolol, nifedipine,
carbamazepine, midazolam, clarithromycin, diclofenac, naproxen, piroxicam, and
oral contraceptives [levonorgestrel/ethinyl estradiol]). In other in
vivostudies, digoxin, ethanol, glyburide, antipyrine, caffeine, metronidazole,
and amoxicillin had no clinically relevant interactions with pantoprazole.
Although no significant drug-drug interactions have been observed in clinical
studies, the potential for significant drug-drug interactions with more than
once-daily dosing with high doses of pantoprazole has not been studied in poor
metabolizers or individuals who are hepatically impaired.
Antacids
There was also no interaction with concomitantly administered antacids.
12.5 Pharmacogenomics
CYP2C19 displays a known genetic polymorphism due to its deficiency in some
subpopulations (e.g., approximately 3% of Caucasians and African-Americans and
17% to 23% of Asians are poor metabolizers). Although these subpopulations of
pantoprazole poor metabolizers have elimination half-life values of 3.5 to 10
hours in adults, they still have minimal accumulation (23% or less) with once-
daily dosing. For adult patients who are CYP2C19 poor metabolizers, no dosage
adjustment is needed.
Similar to adults, pediatric patients who have the poor metabolizer genotype
of CYP2C19 (CYP2C19 *2/*2) exhibited greater than a 6-fold increase in AUC
compared to pediatric extensive (CYP2C19 *1/*1) and intermediate (CYP2C19
*1/*x) metabolizers. Poor metabolizers exhibited approximately 10-fold lower
apparent oral clearance compared to extensive metabolizers.
For known pediatric poor metabolizers, a dose reduction should be considered.
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 24-month carcinogenicity study, Sprague-Dawley rats were treated orally
with pantoprazole doses of 0.5 to 200 mg/kg/day, about 0.1 to 40 times the
exposure on a body surface area basis of a 50 kg person dosed with 40 mg/day.
In the gastric fundus, treatment with 0.5 to 200 mg/kg/day produced
enterochromaffin-like (ECL) cell hyperplasia and benign and malignant
neuroendocrine cell tumors in a dose-related manner. In the forestomach,
treatment with 50 and 200 mg/kg/day (about 10 and 40 times the recommended
human dose on a body surface area basis) produced benign squamous cell
papillomas and malignant squamous cell carcinomas. Rare gastrointestinal
tumors associated with pantoprazole treatment included an adenocarcinoma of
the duodenum with 50 mg/kg/day and benign polyps and adenocarcinomas of the
gastric fundus with 200 mg/kg/day. In the liver, treatment with 0.5 to 200
mg/kg/day produced dose-related increases in the incidences of hepatocellular
adenomas and carcinomas. In the thyroid gland, treatment with 200 mg/kg/day
produced increased incidences of follicular cell adenomas and carcinomas for
both male and female rats.
In a 24-month carcinogenicity study, Fischer 344 rats were treated orally with
doses of 5 to 50 mg/kg/day of pantoprazole, approximately 1 to 10 times the
recommended human dose based on body surface area. In the gastric fundus,
treatment with 5 to 50 mg/kg/day produced enterochromaffin-like (ECL) cell
hyperplasia and benign and malignant neuroendocrine cell tumors. Dose
selection for this study may not have been adequate to comprehensively
evaluate the carcinogenic potential of pantoprazole.
In a 24-month carcinogenicity study, B6C3F1 mice were treated orally with
doses of 5 to 150 mg/kg/day of pantoprazole, 0.5 to 15 times the recommended
human dose based on body surface area. In the liver, treatment with 150
mg/kg/day produced increased incidences of hepatocellular adenomas and
carcinomas in female mice. Treatment with 5 to 150 mg/kg/day also produced
gastric-fundic ECL cell hyperplasia.
A 26-week p53 +/- transgenic mouse carcinogenicity study was not positive.
Pantoprazole was positive in the in vitrohuman lymphocyte chromosomal
aberration assays, in one of two mouse micronucleus tests for clastogenic
effects, and in the in vitroChinese hamster ovarian cell/HGPRT forward
mutation assay for mutagenic effects. Equivocal results were observed in the
in vivorat liver DNA covalent binding assay. Pantoprazole was negative in the
in vitroAmes mutation assay, the in vitrounscheduled DNA synthesis (UDS) assay
with rat hepatocytes, the in vitroAS52/GPT mammalian cell-forward gene
mutation assay, the in vitrothymidine kinase mutation test with mouse lymphoma
L5178Y cells, and the in vivorat bone marrow cell chromosomal aberration
assay.
There were no effects on fertility or reproductive performance when
pantoprazole was given at oral doses up to 500 mg/kg/day in male rats (98
times the recommended human dose based on body surface area) and 450 mg/kg/day
in female rats (88 times the recommended human dose based on body surface
area).
CLINICAL STUDIES SECTION
14 CLINICAL STUDIES
Pantoprazole sodium delayed-release tablets were used in the following clinical trials.
14.1 Erosive Esophagitis (EE) Associated with Gastroesophageal Reflux
Disease (GERD)
Adult Patients
A US multicenter, double-blind, placebo-controlled study of pantoprazole
sodium 10 mg, 20 mg, or 40 mg once daily was conducted in 603 patients with
reflux symptoms and endoscopically diagnosed EE of grade 2 or above (Hetzel-
Dent scale). In this study, approximately 25% of enrolled patients had severe
EE of grade 3, and 10% had grade 4. The percentages of patients healed (per
protocol, n = 541) in this study are shown in Table 8.
Table 8: Erosive Esophagitis Healing Rates (Per Protocol)
|
––––––––––––Pantoprazole sodium––––––––––Placebo | ||||
|
Week |
10 mg daily |
20 mg daily |
40 mg daily |
(n = 68) |
|
4 |
45.6% + |
58.4% +# |
75.0% +* |
14.3% |
|
8 |
66.0% + |
83.5% +# |
92.6% +* |
39.7% |
+ (p < 0.001) pantoprazole sodium versus placebo
- (p < 0.05) versus 10 mg or 20 mg pantoprazole sodium
(p < 0.05) versus 10 mg pantoprazole sodium
In this study, all pantoprazole sodium treatment groups had significantly
greater healing rates than the placebo group. This was true regardless of H.
pyloristatus for the 40 mg and 20 mg pantoprazole sodium treatment groups. The
40 mg dose of pantoprazole sodium resulted in healing rates significantly
greater than those found with either the 20 mg or 10 mg dose.
A significantly greater proportion of patients taking pantoprazole sodium 40
mg experienced complete relief of daytime and nighttime heartburn and the
absence of regurgitation, starting from the first day of treatment, compared
with placebo. Patients taking pantoprazole sodium consumed significantly fewer
antacid tablets per day than those taking placebo.
Pantoprazole sodium 40 mg and 20 mg once daily were also compared with
nizatidine 150 mg twice daily in a US multicenter, double-blind study of 243
patients with reflux symptoms and endoscopically diagnosed EE of grade 2 or
above. The percentages of patients healed (per protocol, n = 212) are shown in
Table 9.
Table 9: Erosive Esophagitis Healing Rates (Per Protocol)
|
–––––––––––––––Pantoprazole sodium–––––––––––––––Nizatidine | |||
|
Week |
20 mgdaily |
40 mg daily |
150 mg twice daily |
|
4 |
61.4% + |
64.0% + |
22.2% |
|
8 |
79.2% + |
82.9% + |
41.4% |
+ (p < 0.001) pantoprazole sodium versus nizatidine
Once-daily treatment with pantoprazole sodium 40 mg or 20 mg resulted in
significantly superior rates of healing at both 4 and 8 weeks compared with
twice-daily treatment with 150 mg of nizatidine. For the 40 mg treatment
group, significantly greater healing rates compared to nizatidine were
achieved regardless of the H. pyloristatus.
A significantly greater proportion of the patients in the pantoprazole sodium
treatment groups experienced complete relief of nighttime heartburn and
regurgitation, starting on the first day and of daytime heartburn on the
second day, compared with those taking nizatidine 150 mg twice daily. Patients
taking pantoprazole sodium consumed significantly fewer antacid tablets per
day than those taking nizatidine.
Pediatric Patients Ages 5 Years through 16 Years
The efficacy of pantoprazole sodium in the treatment of EE associated with
GERD in pediatric patients ages 5 years through 16 years is extrapolated from
adequate and well-conducted trials in adults, as the pathophysiology is
thought to be the same. Four pediatric patients with endoscopically diagnosed
EE were studied in multicenter, randomized, double-blind, parallel-treatment
trials. Children with endoscopically diagnosed EE (defined as an endoscopic
Hetzel-Dent score ≥2) were treated once daily for 8 weeks with one of two dose
levels of pantoprazole sodium (20 mg or 40 mg). All 4 patients with EE were
healed (Hetzel-Dent score of 0 or 1) at 8 weeks.
14.2 Long-Term Maintenance of Healing of Erosive Esophagitis
Two independent, multicenter, randomized, double-blind, comparator-controlled
trials of identical design were conducted in adult GERD patients with
endoscopically confirmed healed EE to demonstrate efficacy of pantoprazole
sodium in long-term maintenance of healing. The two US studies enrolled 386
and 404 patients, respectively, to receive either 10 mg, 20 mg, or 40 mg of
pantoprazole sodium delayed-release tablets once daily or 150 mg of ranitidine
twice daily. As demonstrated in Table 10, pantoprazole sodium 40 mg and 20 mg
were significantly superior to ranitidine at every timepoint with respect to
the maintenance of healing. In addition, pantoprazole sodium 40 mg was
superior to all other treatments studied.
Table 10: Long-Term Maintenance of Healing of Erosive Gastroesophageal
Reflux Disease (GERD Maintenance): Percentage of Patients Who Remained
Healed
|
Pantoprazole sodium |
Pantoprazole sodium 40 mg daily |
Ranitidine | |
|
Study 1 |
n = 75 |
n = 74 |
n = 75 |
|
Month 1 |
91* |
99* |
68 |
|
Month 3 |
82* |
93*# |
54 |
|
Month 6 |
76* |
90*# |
44 |
|
Month 12 |
70* |
86*# |
35 |
|
Study 2 |
n = 74 |
n = 88 |
n = 84 |
|
Month 1 |
89* |
92*# |
62 |
|
Month 3 |
78* |
91*# |
47 |
|
Month 6 |
72* |
88*# |
39 |
|
Month 12 |
72* |
83* |
37 |
- (p <0.05 vs. ranitidine)
(p <0.05 vs. pantoprazole sodium 20 mg)
Note: pantoprazole sodium 10 mg was superior (p < 0.05) to ranitidine in Study 2, but not Study 1.
Pantoprazole sodium 40 mg was superior to ranitidine in reducing the number of
daytime and nighttime heartburn episodes from the first through the twelfth
month of treatment. Pantoprazole sodium 20 mg, administered once daily, was
also effective in reducing episodes of daytime and nighttime heartburn in one
trial, as presented in Table 11.
Table 11: Number of Episodes of Heartburn (mean ± SD)
|
Pantoprazole sodium |
Ranitidine | ||
|
Month 1 |
Daytime |
5.1 ± 1.6* |
18.3 ± 1.6 |
|
Month 12 |
Daytime |
2.9 ± 1.5* |
17.5 ± 1.5 |
- (p <0.001 vs. ranitidine, combined data from the two US studies)
14.3 Pathological Hypersecretory Conditions Including Zollinger-Ellison
Syndrome
In a multicenter, open-label trial of 35 patients with pathological
hypersecretory conditions, such as Zollinger-Ellison Syndrome, with or without
multiple endocrine neoplasia-type I, pantoprazole sodium successfully
controlled gastric acid secretion. Doses ranging from 80 mg daily to 240 mg
daily maintained gastric acid output below 10 mEq/h in patients without prior
acid-reducing surgery and below 5 mEq/h in patients with prior acid-reducing
surgery.
Doses were initially titrated to the individual patient needs, and adjusted in
some patients based on the clinical response with time [see Dosage and Administration ( 2)]. Pantoprazole sodium was well tolerated at these dose
levels for prolonged periods (greater than 2 years in some patients).
INFORMATION FOR PATIENTS SECTION
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication
Guide).
Gastric Malignancy
Advise patients to return to their healthcare provider if they have a
suboptimal response or an early symptomatic relapse [see Warnings and Precautions ( 5.1)].
Acute Tubulointerstitial Nephritis
Advise patients to call their healthcare provider immediately if they
experience signs and/or symptoms associated with acute tubulointerstitial
nephritis [see Contraindications (4), Warnings and Precautions ( 5.2)].
Clostridium difficile-Associated Diarrhea
Advise patients to immediately call their healthcare provider if they
experience diarrhea that does not improve [see Warnings and Precautions ( 5.3)].
Bone Fracture
Advise patients to report any fractures, especially of the hip, wrist or
spine, to their healthcare provider [see Warnings and Precautions ( 5.4)].
Severe Cutaneous Adverse Reactions
Advise patients to discontinue pantoprazole sodium delayed-release tablets and
immediately call their healthcare provider for further evaluation [see Warnings and Precautions ( 5.5)].
Cutaneous and Systemic Lupus Erythematosus
Advise patients to immediately call their healthcare provider for any new or
worsening of symptoms associated with cutaneous or systemic lupus
erythematosus [see Warnings and Precautions ( 5.6)].
Cyanocobalamin (Vitamin B-12) Deficiency
Advise patients to report any clinical symptoms that may be associated with
cyancobalamin deficiency to their healthcare provider if they have been
receiving pantoprazole sodium delayed-release tablets for longer than 3 years
[see Warnings and Precautions ( 5.7)].
Hypomagnesemia and Mineral Metabolism
Advise patients to report any clinical symptoms that may be associated with
hypomagnesemia, hypocalcemia, and/or hypokalemia, to their healthcare
provider, if they have been receiving pantoprazole sodium delayed-release
tablets for at least 3 months [see Warnings and Precautions ( 5.8)].
Drug Interactions
Instruct patients to inform their healthcare provider of any other medications
they are currently taking, including rilpivirine-containing products [see Contraindications (4)],digoxin [see Warnings and Precautions ( 5.8)] and high
dose methotrexate [see Warnings and Precautions ( 5.13)].
Pregnancy
Advise a pregnant woman of the potential risk to a fetus. Advise females of
reproductive potential to inform their healthcare provider of a known or
suspected pregnancy [see Use in Specific Populations ( 8.1)].
Administration
• Do not split, crush, or chew pantoprazole sodium delayed-release tablets.
• Swallow pantoprazole sodium delayed-release tablets whole, with or without
food in the stomach.
• Concomitant administration of antacids does not affect the absorption of
pantoprazole sodium delayed-release tablets.
• Take a missed dose as soon as possible. If it is almost time for the next
dose, skip the missed dose and take the next dose at the regular scheduled
time. Do not take 2 doses at the same time.
Relabeled and Repackaged by:
Enovachem PHARMACEUTICALS
Torrance, CA 90501