
Naloxone Hydrochloride
Naloxone Hydrochloride Injection, USP USP type-I clear tubular glass Vial, Opioid Antagonist Protect from light by retaining in the carton until ready for use. Discard unused portion. Rx only
dfa48492-d83b-48cc-9ad1-bdc0c2ac9931
HUMAN PRESCRIPTION DRUG LABEL
Dec 18, 2023
Somerset Therapeutics, LLC
DUNS: 079947873
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Naloxone Hydrochloride
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (4)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
1 mL Container Label

1 mL Carton Label
ADVERSE REACTIONS SECTION
ADVERSE REACTIONS
Postoperative
The following adverse events have been associated with the use of naloxone hydrochloride injection in postoperative patients: hypotension, hypertension, ventricular tachycardia and fibrillation, dyspnea, pulmonary edema, and cardiac arrest. Death, coma, and encephalopathy have been reported as sequelae of these events. Excessive doses of naloxone in postoperative patients may result in significant reversal of analgesia and may cause agitation (see PRECAUTIONSandDOSAGE AND ADMINISTRATION; Usage in Adults; Postoperative Opioid Depression).
Opioid Depression
Abrupt reversal of opioid depression may result in nausea, vomiting, sweating, tachycardia, increased blood pressure, tremulousness, seizures, ventricular tachycardia and fibrillation, pulmonary edema, and cardiac arrest which may result in death (seePRECAUTIONS).
Opioid Dependence
Abrupt reversal of opioid effects in persons who are physically dependent on opioids may precipitate an acute withdrawal syndrome which may include, but is not limited to the following signs and symptoms: body aches, fever, sweating, runny nose, sneezing, piloerection, yawning, weakness, shivering or trembling, nervousness, restlessness or irritability, diarrhea, nausea or vomiting, abdominal cramps, increased blood pressure, and tachycardia. In the neonate, opioid withdrawal may also include: convulsions, excessive crying, and hyperactive reflexes (SeeWARNINGS).
Adverse events associated with the postoperative use of naloxone hydrochloride injection are listed by organ system and in decreasing order of frequency as follows:
Cardiac Disorders: pulmonary edema, cardiac arrest or failure, tachycardia, ventricular fibrillation, and ventricular tachycardia. Death, coma, and encephalopathy have been reported as sequelae of these events.
Gastrointestinal Disorders: vomiting, nausea
Nervous System Disorders: convulsions, paraesthesia, grand mal convulsion
Psychiatric Disorders: agitation, hallucination, tremulousness
Respiratory, Thoracic, and Mediastinal Disorders: dyspnea, respiratory depression, hypoxia
Skin and Subcutaneous Tissue Disorders: nonspecific injection site reactions, sweating
Vascular Disorders: hypertension, hypotension, hot flashes or flushing
SeePRECAUTIONSand** DOSAGE AND ADMINISTRATION; Usage in Adults, Postoperative Opioid Depression.**
DESCRIPTION SECTION
DESCRIPTION
Naloxone Hydrochloride Injection, USP is a sterile, nonpyrogenic solution of naloxone hydrochloride in water for injection. Each milliliter (mL) contains 0.4 mg naloxone hydrochloride and sodium chloride to adjust tonicity in water for injection. May contain hydrochloric acid for pH adjustment; pH 4.0 (3.0 to 6.5).
The single-dose solution contains no bacteriostat, antimicrobial agent or added buffer (except for pH adjustment) and is intended for use only as a single-dose injection. When smaller doses are required, the unused portion should be discarded.
Naloxone Hydrochloride Injection, USP may be administered intravenously, intramuscularly, or subcutaneously.
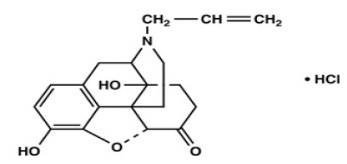
Naloxone, an opioid antagonist, is a synthetic congener of oxymorphone. It differs from oxymorphone in that the methyl group on the nitrogen atom is replaced by an allyl group.
Naloxone Hydrochloride, USP is chemically designated 17-Allyl-4,5α-epoxy-3,14-dihydroxymorphinan-6-one hydrochloride (C19H21NO4 • HCl), a white to slightly off-white powder soluble in water, in dilute acids, and in strong alkali; slightly soluble in alcohol; practically insoluble in ether and chloroform. It has a molecular weight of 363.84. It has the following structural formula:
CLINICAL PHARMACOLOGY SECTION
CLINICAL PHARMACOLOGY
Complete or Partial Reversal of Opioid Depression
Naloxone prevents or reverses the effects of opioids including respiratory depression, sedation and hypotension. Also, Naloxone can reverse the psychotomimetic and dysphoric effects of agonist-antagonists such as pentazocine.
Naloxone is an essentially pure opioid antagonist, i.e., it does not possess the "agonistic" or morphine-like properties characteristic of other opioid antagonists. When administered in usual doses and in the absence of opioids or agonistic effects of other opioid antagonists, it exhibits essentially no pharmacologic activity.
Naloxone has not been shown to produce tolerance or cause physical or psychological dependence. In the presence of physical dependence on opioids, naloxone will produce withdrawal symptoms. However, in the presence of opioid dependence, opiate withdrawal symptoms may appear within minutes of naloxone administration and will subside in about 2 hours. The severity and duration of the withdrawal syndrome are related to the dose of naloxone and to the degree and type of opioid dependence.
While the mechanism of action of naloxone is not fully understood, in vitro evidence suggests that naloxone antagonizes opioid effects by competing for the mu, kappa, and sigma opiate receptor sites in the CNS, with the greatest affinity for the mu receptor.
When naloxone hydrochloride is administered intravenously, the onset of action is generally apparent within two minutes; the onset of action is slightly less rapid when it is administered subcutaneously or intramuscularly. The duration of action is dependent upon the dose and route of administration of naloxone hydrochloride. Intramuscular administration produces a more prolonged effect than intravenous administration. Since the duration of action of naloxone may be shorter than that of some opiates, the effects of the opiate may return as the effects of naloxone dissipates.
The requirement for repeat doses of naloxone, however, will also be dependent upon the amount, type and route of administration of the opioid being antagonized.
Adjunctive Use in Septic Shock
Naloxone has been shown in some cases of septic shock to produce a rise in blood pressure that may last up to several hours; however this pressor response has not been demonstrated to improve patient survival. In some studies, treatment with naloxone in the setting of septic shock has been associated with adverse effects, including agitation, nausea and vomiting, pulmonary edema, hypotension, cardiac arrhythmias, and seizures. The decision to use naloxone in septic shock should be exercised with caution, particularly in patients who may have underlying pain or have previously received opioid therapy and may have developed opioid tolerance.
Because of the limited number of patients who have been treated, optimal dosage and treatment regimens have not been established.
PHARMACOKINETICS SECTION
PHARMACOKINETICS
Distribution
Following parenteral administration, naloxone is rapidly distributed in the body and readily crosses the placenta. Plasma protein binding occurs but is relatively weak. Plasma albumin is the major binding constituent but significant binding of naloxone also occurs to plasma constituents other than albumin. It is not known whether naloxone is excreted into human milk.
Metabolism and Elimination
Naloxone is metabolized in the liver primarily by glucuronide conjugation with naloxone-3-glucuronide as the major metabolite. In one study, the serum half- life in adults ranged from 30 to 81 minutes (mean 64 ± 12 minutes). In a neonatal study, the mean plasma half-life was observed to be 3.1 ± 0.5 hours. After an oral or intravenous dose, about 25 to 40% of the drug is excreted as metabolites in urine within 6 hours, about 50% in 24 hours, and 60 to 70% in 72 hours.
WARNINGS SECTION
WARNINGS
Drug Dependence
Naloxone hydrochloride injection should be administered cautiously to persons, including newborns of mothers, who are known or suspected to be physically dependent on opioids. In such cases an abrupt and complete reversal of opioid effects may precipitate an acute withdrawal syndrome.
The signs and symptoms of opioid withdrawal in a patient physically dependent on opioids may include, but are not limited to, the following: body aches, diarrhea, tachycardia, fever, runny nose, sneezing, piloerection, sweating, yawning, nausea or vomiting, nervousness, restlessness or irritability, shivering or trembling, abdominal cramps, weakness, and increased blood pressure. In the neonate, opioid withdrawal may also include: convulsions, excessive crying, and hyperactive reflexes.
Repeat Administration
The patient who has satisfactorily responded to naloxone should be kept under continued surveillance and repeated doses of naloxone should be administered, as necessary, since the duration of action of some opioids may exceed that of naloxone.
Respiratory Depression Due to Other Drugs
Naloxone is not effective against respiratory depression due to non-opioid drugs and in the management of acute toxicity caused by levopropoxyphene. Reversal of respiratory depression by partial agonists or mixed agonist/antagonists, such as buprenorphine and pentazocine, may be incomplete or require higher doses of naloxone. If an incomplete response occurs, respirations should be mechanically assisted as clinically indicated.
OVERDOSAGE SECTION
OVERDOSAGE
There is limited clinical experience with naloxone hydrochloride injection overdosage in humans.
Adult Patients
In one small study, volunteers who received 24 mg/70 kg did not demonstrate toxicity.
In another study, 36 patients with acute stroke received a loading dose of 4 mg/kg (10 mg/m2/min) of naloxone hydrochloride injection followed immediately by 2 mg/kg/hr for 24 hours. Twenty-three patients experienced adverse events associated with naloxone use, and naloxone was discontinued in seven patients because of adverse effects. The most serious adverse events were: seizures (2 patients), severe hypertension (1), and hypotension and/or bradycardia (3).
At doses of 2 mg/kg in normal subjects, cognitive impairment and behavioral symptoms, including irritability, anxiety, tension, suspiciousness, sadness, difficulty concentrating, and lack of appetite have been reported. In addition, somatic symptoms, including dizziness, heaviness, sweating, nausea, and stomachaches were also reported. Although complete information is not available, behavioral symptoms were reported to often persist for 2 to 3 days.
Pediatric Patients
Up to 11 doses of 0.2 mg naloxone (2.2 mg) have been administered to children following overdose of diphenoxylate hydrochloride with atropine sulfate. Pediatric reports include a 2½ year-old child who inadvertently received a dose of 20 mg naloxone for treatment of respiratory depression following overdose with diphenoxylate hydrochloride with atropine sulfate. The child responded well and recovered without adverse sequelae. There is also a report of a 4½ year-old child who received 11 doses during a 12-hour period, with no adverse sequelae.
Patient Management
Patients who experience a naloxone overdose should be treated symptomatically in a closely supervised environment. Physicians should contact a poison control center for the most up-to-date patient management information.
HOW SUPPLIED SECTION
HOW SUPPLIED
Naloxone Hydrochloride Injection, USP is a clear, colorless solution.
Naloxone Hydrochloride Injection, USP for intravenous, intramuscular, and subcutaneous administration is available as:
|
** NDC Number** |
** Container** |
** Concentration** |
|
70069-** 071** -10 |
Single-dose Fliptop Vial |
0.4 mg/ 1 mL (0.4 mg/mL) |
1 mL vials are Single Dose Vials, packaged 10 vials per carton.
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature].
Protect from light.
Store in the carton until contents have been used.
Discard unused portion.
For Product Inquiry call 1-800-417-9175.
ST-NLX11/P/02
Revised: October, 2019
Manufactured for:
Somerset Therapeutics, LLC
Hollywood, FL 33024
Made in India
Code No.: KR/DRUGS/KTK/28/289/97