
Regulatory Information
HSA regulatory responsibility and product classification details
Regulatory Responsibility
Product Classification
Formulation Information
INFUSION, SOLUTION
**Posology and method of administration** Posology The dose and posology is dependent on the indication. In replacement therapy, the dose may need to be individualised for each patient dependent on the pharmacokinetic and clinical response. The following dose regimens are given as a guideline. _Replacement therapy in primary immunodeficiency syndromes_ The dose should achieve a trough level of IgG (measured before the next infusion) of at least 4 – 6 g/l. Three to six months are required after the initiation of therapy for equilibration to occur. The recommended starting dose is 0.4 – 0.8 g/kg followed by at least 0.2 g/kg/month given in divided doses every three to four weeks. The dose required to achieve a trough level of 6 g/l is of the order of 0.2 – 0.8 g/kg/month. The dose interval when steady state has been reached varies from 3 – 4 weeks. Trough levels should be measured and assessed in conjuction with the incidence of infection. To reduce the rate of infection, it may be necessary to increase the dosage and aim for higher trough levels (> 6 – 9 g/l). _Hypogammaglobulinaemia and recurrent bacterial infections in patients with chronic lymphocytic leukaemia, in whom prophylactic antibiotics have failed; hypogammaglobulinaemia and recurrent bacterial infections in plateau phase multiple myeloma patients who have failed to respond to pneumococcal immunisation; children and adolescents with congenital AIDS and recurrent bacterial infections_ The recommended dose is 0.2 – 0.4 g/kg every three to four weeks. _Hypogammaglobulinaemia in patients after allogenic haematopoietic stem cell transplantation_ The recommended dose is 0.2 – 0.4 g/kg every three to four weeks. The trough levels should be maintained above 5 g/l. _Idiopathic Thrombocytopenic Purpura_ For the treatment of an acute episode, 0.8 – 1 g/kg on day one, which may be repeated once within 3 days, or 0.4 g/kg daily for two to five days. The treatment can be repeated if relapse occurs. _Guillain Barré syndrome_ 0.4 g/kg/day for 5 days. _Kawasaki disease_ 1.6 – 2.0 g/kg should be administered in divided doses over two to five days or 2.0 g/kg as a single dose. Patients should receive concomitant treatment with acetylsalicylic acid. The dose recommendations are summarised in the following table: 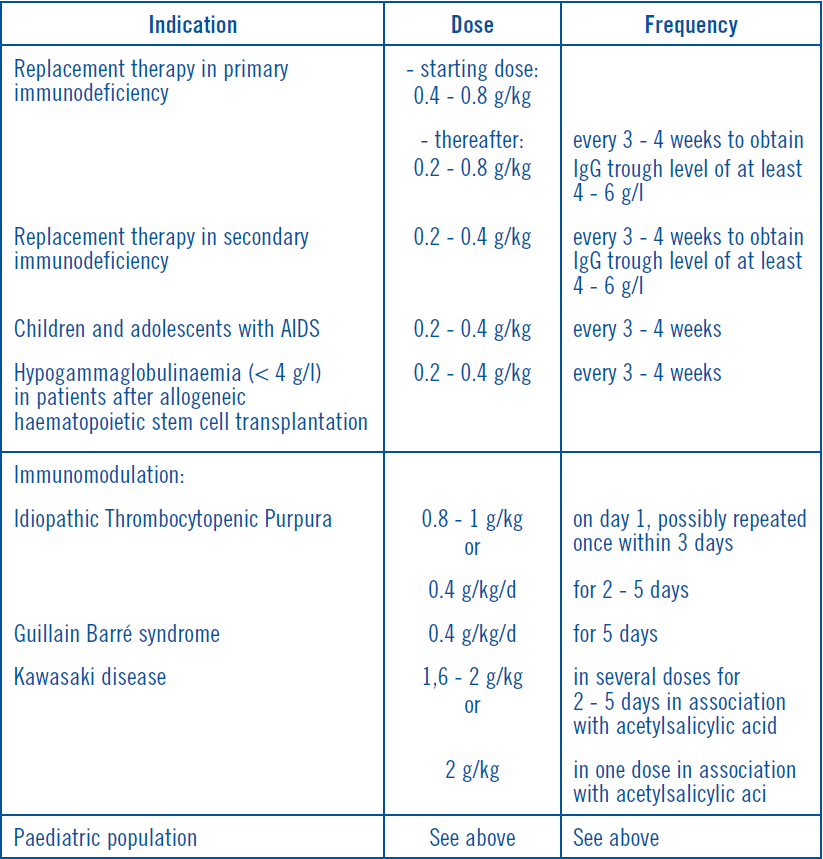 _Paediatric population_ The safety and efficacy of Flebogamma® 10% DIF in children and adolescents aged 3 to 16 years have been established in 3 primary immunodeficient patients and in 9 patients with immune thrombocytopenic purpura. The safety and efficacy of Flebogamma® 10% DIF in children aged 0 to 2 years have not been established in clinical trials. As the posology for each indication is given by body weight and adjusted to the clinical outcome of the above mentioned conditions, the posology in children is not considered to be different to that of adults. Method of administration Flebogamma® 10% DIF should be infused intravenously at an initial rate of 0.01 ml/kg/min for the first thirty minutes. If tolerated, advance to 0.02 ml/kg/min for the second 30 minutes. Again, if tolerated, advance to 0.04 ml/kg/min for the third 30 minutes. If the patient tolerates the infusion well, additional increments of 0.02 ml/kg/min may be made at 30-minute intervals up to a maximum of 0.08 ml/kg/min. It has been reported that the frequency of adverse reactions to IVIg increases with the infusion rate. Infusion rates during the initial infusions should be slow. If there are no adverse reactions, the infusion rate for subsequent infusions can be slowly increased to the maximum rate. For patients experiencing adverse reactions, it is advisable to reduce the infusion rate in subsequent infusions and limit the maximum rate to 0.04 ml/kg/min or administer IVIg at a 5% concentration (see section “Special warnings and precautions for use” – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_).
INTRAVENOUS
Medical Information
**Therapeutic indications** Replacement therapy in adults, children and adolescents (2–18 years) in: - Primary immunodeficiency syndromes with impaired antibody production. - Hypogammaglobulinaemia and recurrent bacterial infections in patients with chronic lymphocytic leukaemia, in whom prophylactic antibiotics have failed. - Hypogammaglobulinaemia and recurrent bacterial infections in plateau phase multiple myeloma patients who failed to respond to pneumococcal immunisation. - Hypogammaglobulinaemia in patients after allogenic haematopoietic stem cell transplantation (HSCT). Replacement therapy in children and adolescents (2–18 years) in: - Congenital AIDS with recurrent bacterial infections. Immunomodulation in adults, children and adolescents (2–18 years) in: - Idiopathic Thrombocytopenic Purpura (ITP), in patients at high risk of bleeding or prior to surgery to correct the platelet count. - Guillain Barré syndrome. - Kawasaki disease.
**Contraindications** Hypersensitivity to the active substance or to any of the excipients (see section “Special warnings and precautions for use” – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). Hypersensitivity to human immunoglobulins, especially in very rare cases of IgA deficiency, when the patient has antibodies against IgA. Hereditary fructose intolerance (see section “Special warnings and precautions for use” – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). **In babies and young children hereditary fructose intolerance may not yet be diagnosed and may be fatal, thus, they should not receive this medicinal product.**
J06BA02
immunoglobulins, normal human, for intravascular adm.
Manufacturer Information
GRIFOLS ASIA PACIFIC PTE. LTD.
INSTITUTO GRIFOLS, S.A.
Active Ingredients
Documents
Package Inserts
Flebogamma DIF 10% final PI.pdf
Approved: June 14, 2012