
Regulatory Information
HSA regulatory responsibility and product classification details
Regulatory Responsibility
Product Classification
Formulation Information
TABLET
**Dosage** The dosage is based on the desired effect and on how the patient tolerates the medicine. Therapy with Tritace is usually long-term therapy; the doctor determines the duration of treatment individually for each patient. _Treatment of hypertension_ The recommended initial dose is 2.5 mg once daily. Depending on the response, the dose may be increased. Any increase should be implemented by doubling the dose at intervals of 2 to 3 weeks. The usual maintenance dose is 2.5 to 5 mg daily, the maximum dose is 10 mg daily. In impaired renal function, i.e., a creatinine clearance between 50 and 20 ml/min per 1.73 m2 body surface area, the initial dose is generally 1.25 mg and the maximum daily dose is 5 mg. When creatinine clearance cannot be measured, it can be calculated based on the serum creatinine level using the following formula (Cockcroft’s equation): 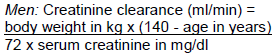 _Women:_ Multiply the product of the above equation by 0.85. In patients with incompletely corrected fluid or salt deficiency, those with severe hypertension, as well as in those for whom a hypotensive reaction would constitute a particular risk (e.g. patients with haemodynamically relevant stenoses of the coronary arteries or of the blood vessels supplying the brain) and in the elderly, a reduced initial dose of 1.25 mg daily must be considered. In patients pre-treated with a diuretic, consideration must be given to discontinuing the diuretic for at least 2 to 3 days or – depending on the duration of action of the diuretic – longer before starting treatment with Tritace, or at least to reducing the diuretic dose. The doctor will decide in each individual case whether such discontinuation or dose reduction is possible and how long it should last. The initial dose in such patients is generally 1.25 mg Tritace. In impaired liver function, response to treatment may be either increased or reduced. Therefore, treatment must be initiated only under close medical supervision. The maximum daily dose is 2.5 mg. _Treatment of congestive heart failure_ The recommended initial dose is 1.25 mg once daily. Depending on the response, the dose may be increased. Any increase should be implemented by doubling the dose at intervals of 1 to 2 weeks. The maximum daily dose is 10 mg. The required daily dose, if equalling or exceeding 2.5 mg, may be taken as a single dose or in two separate doses. In impaired liver or renal function and in patients pre-treated with a diuretic, dosage recommendations for Tritace are identical to those given above in _Treatment of hypertension_. The recommendations given there in conjunction with diuretic pre-treatment also apply. _Treatment after myocardial infarction_ The recommended initial dose is 5 mg daily, divided into two single doses of 2.5 mg each, one in the morning and one in the evening. If this dose is not well tolerated, 1.25 mg should be taken twice daily over two days. In either event, depending on the response, the dose may then be increased. If the dose cannot be increased to 2.5mg twice a day treatment should be withdrawn. Any increase should be implemented by doubling the dose at intervals of 1 to 3 days. As treatment progresses, the total daily dose may be taken as a single dose. The maximum daily dose is 10 mg. Sufficient experience is still lacking in the treatment of patients with severe (NYHA IV) heart failure immediately after myocardial infarction. Treatment, if nevertheless given, should be started with 1.25 mg once daily, and increased only with particular caution. In patients with impaired liver or renal function, with incompletely corrected fluid or salt deficiency, or with severe hypertension, and in those for whom a hypotensive reaction would constitute a particular risk (e.g. patients with haemodynamically relevant stenoses of the coronary arteries or of the blood vessels supplying the brain), as well as in those pre-treated with a diuretic and in the elderly, the recommendations are identical to those given above in _Treatment of hypertension_. _Reducing the risk of myocardial infarction, stroke or cardiovascular death and/or the need for revascularisation procedures:_ The recommended initial dose is 2.5 mg once daily. Depending on the tolerability, the dose is gradually increased. The increase should be implemented by doubling the dose after one week. Three weeks later, it should be doubled again to the usual maintenance dose of 10 mg. In patients with impaired liver or renal function, with incompletely corrected fluid or salt deficiency, or with severe hypertension, and in those for whom a hypotensive reaction would constitute a particular risk (e.g. patients with haemodynamically relevant stenoses of the coronary arteries or of the blood vessels supplying the brain), as well as in those pre-treated with a diuretic and in the elderly, the recommendations are identical to those given above in _Treatment of hypertension_. _Progressive renal failure in patients with persistent proteinuria in excess of 1g/day_ The recommended initial dose is 1.25mg Tritace once daily. This should be doubled at intervals of 2–3 weeks, depending on how the drug is tolerated. There are no efficacy data regarding doses above 5mg/day in patients with nephropathy. In hypertensive patients, a target diastolic blood pressure of < 90mm Hg should be pursued. In patients pre-treated with a diuretic, consideration must be given to discontinuing the diuretic for at least 2–3 days or longer (depending on duration of action) or at least consideration should be given to reducing the dose, before initiating Tritace.
ORAL
Medical Information
**Indications** - Hypertension - Congestive heart failure - Treatment of patients who – within the first few days after an acute myocardial infarction – have demonstrated clinical signs of congestive heart failure - For reducing the risk of myocardial infarction, stroke, cardiovascular death or need for revascularisation procedures in patients of 55 years or more who have clinical evidence of cardiovascular disease (previous MI, unstable angina or multivessel CABG or multivessel PTCA), stroke or peripheral vascular disease. - For reducing the risk of myocardial infarction, stroke, cardiovascular death or need for revascularisation procedures in diabetic patients of 55 years or more who have one or more of the following clinical findings: hypertension (systolic blood pressure > 160mmHg or diastolic blood pressure > 90mmHg); high total cholesterol (>5.2 mmol/L); low HDL (<0.9 mmol/L); current smoker; known microalbuminuria; clinical evidence of previous vascular disease. - Prevention of progressive renal failure in patients with persistent proteinuria in excess of 1g/day
**Contraindications** Tritace must not be used in patients with - hypersensitivity to ramipril, any other ACE inhibitor, or to any of the excipients (see “Composition” – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_) - a history of angioedema (risk of precipitating angioedema; see also “Adverse reactions” – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_) - concomitantly with sacubitril/valsartan therapy (see “Interaction” – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). Do not initiate Tritace until sacubitril/valsartan is eliminated from the body. In case of switch from Tritace to sacubitril/valsartan, do not start sacubitril/valsartan until Tritace is eliminated from the body. - blood-flow-reducing narrowing (haemodynamically relevant stenosis) of the renal artery, bilateral or unilateral in the single kidney (risk of fall in blood pressure and renal failure) - low blood pressure or labile circulatory condition (risk of fall in blood pressure and renal failure). Since severe rapid-onset and allergy-like (anaphylactoid) hypersensitivity reactions may occur, treatment with ACE inhibitors in conjunction with extracorporeal treatments leading to contact of blood with negatively charged surfaces must be avoided. The latter include dialysis or haemofiltration with certain high-flux membranes (e.g. polyacrylonitril membranes) and low-density lipoprotein apheresis with dextran sulfate. - concomitant use of aliskiren-containing medicines in patients with diabetes or with moderate to severe renal impairment (creatinine clearance < 60 ml/min) - during pregnancy - with angiotensin II receptor blockers in patients with diabetic nephropathy
C09AA05
ramipril
Manufacturer Information
SANOFI-AVENTIS SINGAPORE PTE. LTD.
SANOFI S.r.l.
Active Ingredients
Documents
Package Inserts
Tritace PI_Approved.pdf
Approved: April 26, 2022