
Regulatory Information
HSA regulatory responsibility and product classification details
Regulatory Responsibility
Product Classification
Formulation Information
INFUSION, SOLUTION CONCENTRATE
**Dosage and Administration** DARZALEX® should be administered by a healthcare professional, with immediate access to emergency equipment and appropriate medical support to manage infusion-related reactions (IRRs) if they occur. Pre- and post-infusion medications should be administered (see _Recommended concomitant medications_ below). **Dosage – Adults (≥18 years)** _**Recommended dose**_ The DARZALEX® dosing schedule in Table 1 is for combination therapy with 4-week cycle regimens (e.g. lenalidomide) and for monotherapy as follows: - combination therapy with lenalidomide and low-dose dexamethasone for patients with newly diagnosed multiple myeloma ineligible for autologous stem cell transplant (ASCT) - combination therapy with lenalidomide and low-dose dexamethasone for patients with relapsed/refractory multiple myeloma - combination therapy with carfilzomib and low-dose dexamethasone for patients with relapsed/refractory multiple myeloma - monotherapy for patients with relapsed/refractory multiple myeloma The recommended dose is DARZALEX® 16 mg/kg body weight administered as an intravenous infusion according to the following dosing schedule (infusion rates presented in Table 5): 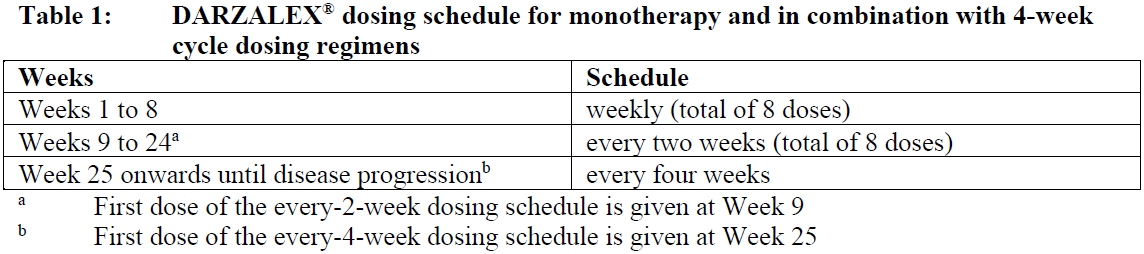 For dosing instructions of medicinal products administered with DARZALEX®, see _Clinical Studies_ and manufacturer’s prescribing information – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_. The DARZALEX® dosing schedule in Table 2 is for combination therapy with bortezomib, melphalan and prednisone (6-week cycle regimen) for patients with newly diagnosed multiple myeloma ineligible for ASCT. The recommended dose is DARZALEX® 16 mg/kg body weight administered as an intravenous infusion according to the following dosing schedule (infusion rates presented in Table 5): 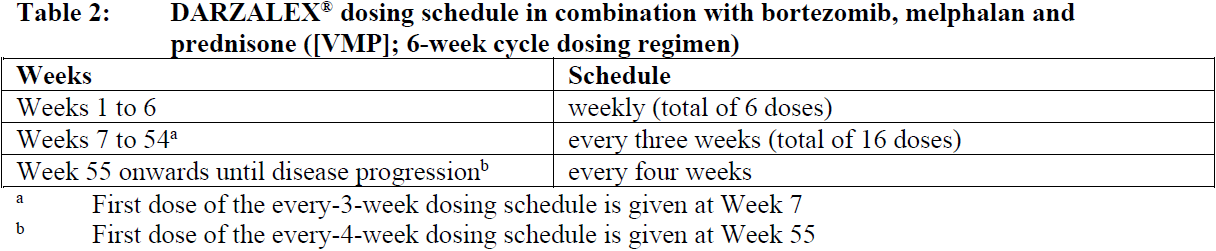 Bortezomib is given twice weekly at Weeks 1, 2, 4 and 5 for the first 6-week cycle, followed by **once** weekly at Weeks 1, 2, 4 and 5 for eight more 6-week cycles. For information on the VMP dose and dosing schedule when administered with DARZALEX®, see _Clinical Studies_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_. The DARZALEX® dosing schedule in Table 3 is for combination therapy with bortezomib, thalidomide and dexamethasone (4-week cycle regimens) for treatment of newly diagnosed patients eligible for ASCT. The recommended dose is DARZALEX® 16mg/kg body weight administered as an intravenous infusion according to the following dosing schedule (infusion rates presented in Table 5): 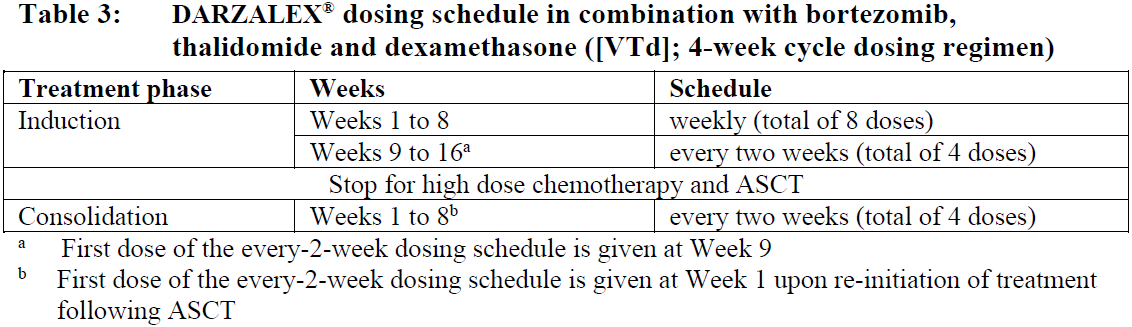 For dosing instructions of medicinal products administered with DARZALEX®, see Clinical Studies and manufacturer’s prescribing information – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_. The DARZALEX® dosing schedule in Table 4 is for combination therapy with 3-week cycle regimens (e.g. bortezomib) for patients with relapsed/refractory multiple myeloma. The recommended dose is DARZALEX® 16 mg/kg body weight administered as an intravenous infusion according to the following dosing schedule (infusion rates presented in Table 5):  For dosing instructions for medicinal products administered with DARZALEX®, see _Clinical Studies_ and manufacturer’s prescribing information – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_. _**Missed dose (s)**_ If a planned dose of DARZALEX® is missed, administer the dose as soon as possible and adjust the dosing schedule accordingly, maintaining the treatment interval. _**Dose modifications**_ No dose reduction of DARZALEX® are recommended. Dose delay may be required to allow recovery of blood cell counts in the event of hematological toxicity (see _Warnings and Precautions_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). For information concerning medicinal products given in combination with DARZALEX®, see manufacturer’s prescribing information. **_Recommended concomitant medications_** _**Pre-infusion medication**_ Administer the following pre-infusion medications to reduce the risk of IRRs to all patients 1–3 hours prior to every infusion of DARZALEX®: - Corticosteroid (long-acting or intermediate-acting) **Monotherapy:** Methylprednisolone 100 mg, or equivalent, administered intravenously. Following the second infusion, the dose of corticosteroid may be reduced (oral or intravenous methylprednisolone 60 mg). **Combination therapy:** Administer 20 mg dexamethasone (or equivalent) prior to every DARZALEX® infusion. When dexamethasone is the background-regimen specific corticosteroid, the dexamethasone treatment dose will instead serve as pre-medication on DARZALEX® infusion days (see _Clinical Studies_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). Dexamethasone is given intravenously prior to the first DARZALEX® infusion and oral administration may be considered prior to subsequent infusions. Additional background-regimen specific corticosteroids (e.g. prednisone) should not be taken on DARZALEX® infusion days when patients have received dexamethasone as a pre-medication. - Antipyretics (oral paracetamol/acetaminophen 650 to 1000 mg). - Antihistamine (oral or intravenous diphenhydramine 25 to 50 mg or equivalent). _**Post-infusion medication**_ Administer post-infusion medication to reduce the risk of delayed infusion-related reactions as follows: - **Monotherapy:** Administer oral corticosteroid (20 mg methylprednisolone or equivalent dose of an intermediate-acting or long-acting corticosteroid in accordance with local standards) on each of the 2 days following all DARZALEX® infusions (beginning the day after the infusion). - **Combination therapy:** Consider administering low-dose oral methylprednisolone (≤ 20 mg) or equivalent the day after the DARZALEX® infusion. However, if a background regimen-specific corticosteroid (e.g. dexamethasone, prednisone) is administered the day after the DARZALEX® infusion, additional post-infusion medications may not be needed (see _Clinical Studies_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). Additionally, for patients with a history of chronic obstructive pulmonary disease, consider the use of post-infusion medications including short and long acting bronchodilators, and inhaled corticosteroids. Following the first four infusions, if the patient experiences no major IRRs, these inhaled post-infusion medications may be discontinued at the discretion of the physician. _Prophylaxis for herpes zoster virus reactivation_ Anti-viral prophylaxis should be considered for the prevention of herpes zoster virus reactivation. If required, anti-viral prophylaxis is recommended to be initiated within 1 week of starting DARZALEX®. **Special populations** _**Pediatrics (17 years of age and younger)**_ The safety and efficacy of DARZALEX® have not been established in pediatric patients. _**Elderly (65 years of age and older)**_ No dose adjustments are considered necessary in elderly patients (see _Pharmacokinetic Properties, Adverse Reactions_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). _**Renal impairment**_ No formal studies of daratumumab in patients with renal impairment have been conducted. Based on population pharmacokinetic (PK) analyses, no dosage adjustment is necessary for patients with renal impairment (see _Pharmacokinetic Properties_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). _**Hepatic impairment**_ No formal studies of daratumumab in patients with hepatic impairment have been conducted. Changes in hepatic function are unlikely to have any effect on the elimination of daratumumab since IgG1 molecules such as daratumumab are not metabolized through hepatic pathways. Based on population PK analyses, no dosage adjustments are necessary for patients with hepatic impairment (see _Pharmacokinetic Properties_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). **Administration** DARZALEX® is administered as an intravenous infusion following dilution with 0.9% Sodium Chloride. For instructions on dilution of the medicinal product before administration, see _Instructions for Use and Handling and Disposal_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_. Following dilution the DARZALEX® infusion should be intravenously administered at the appropriate initial infusion rate, presented in Table 5 below. Incremental escalation of the infusion rate should be considered only in the absence of infusion reactions. To facilitate administration, the first prescribed 16 mg/kg dose at Week 1 may be split over two consecutive days i.e. 8 mg/kg on Day 1 and Day 2 respectively, see Table 5 below. For patients receiving DARZALEX® in combination with carfilzomib and dexamethasone (DKd), 16 mg/kg daratumumab dose at Week 1 should be split over two days to minimize risk of volume overload (See option 2 Table 5). 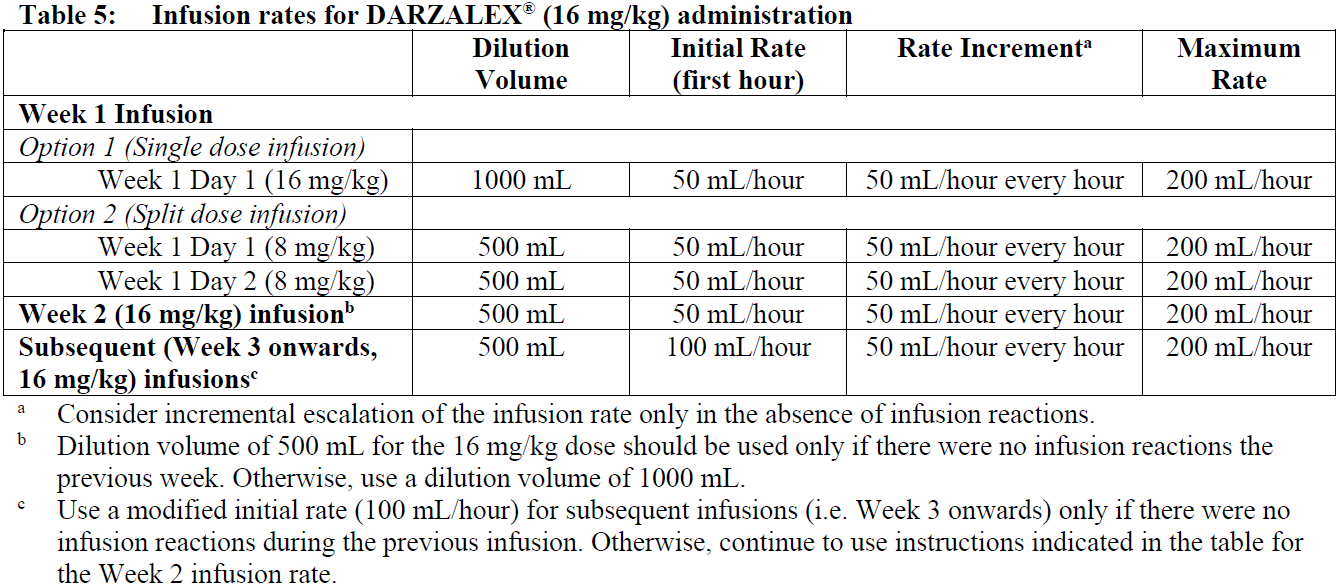 **Management of infusion-related reactions** Administer pre-infusion medications to reduce the risk of IRRs prior to treatment with DARZALEX®. For IRRs of any grade/severity, immediately interrupt the DARZALEX® infusion and manage symptoms. Management of IRRs may further require reduction in the rate of infusion, or treatment discontinuation of DARZALEX® as outlined below (see also _Warnings and Precautions_ – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_). - Grade 1–2 (mild to moderate): Once reaction symptoms resolve, resume the infusion at no more than half the rate at which the IRR occurred. If the patient does not experience any further IRR symptoms, infusion rate escalation may resume at increments and intervals as clinically appropriate up to the maximum rate of 200 mL/hour (Table 5). - Grade 3 (severe): Once reaction symptoms resolve, consider restarting the infusion at no more than half the rate at which the reaction occurred. If the patient does not experience additional symptoms, resume infusion rate escalation at increments and intervals as appropriate (Table 5). Repeat the procedure above in the event of recurrence of Grade 3 symptoms. Permanently discontinue DARZALEX® upon the third occurrence of a Grade 3 or greater infusion reaction. - Grade 4 (life-threatening): Permanently discontinue DARZALEX® treatment.
INTRAVENOUS
Medical Information
**Indications** DARZALEX® is indicated for the treatment of patients with multiple myeloma: - in combination with bortezomib, melphalan and prednisone, or in combination with lenalidomide and dexamethasone in newly diagnosed patients who are ineligible for autologous stem cell transplant. - in combination with bortezomib, thalidomide and dexamethasone in newly diagnosed patients who are eligible for autologous stem cell transplant. - in combination with lenalidomide and dexamethasone, or in combination with bortezomib and dexamethasone in patients who have received at least one prior therapy. - in combination with carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma who have received one to three prior lines of therapy. - as monotherapy, in patients who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent.
**Contraindications** Patients with a history of severe hypersensitivity to daratumumab or any of the excipients.
L01XC24
xl 01 xc 24
Manufacturer Information
JOHNSON & JOHNSON INTERNATIONAL (SINGAPORE) PTE. LTD.
Cilag A.G.
Vetter Pharma-Fertigung GmbH & Co. KG
Active Ingredients
Documents
Package Inserts
Darzalex IV PI.pdf
Approved: April 19, 2023