
Flurbiprofen
These highlights do not include all the information needed to use FLURBIPROFEN TABLETS safely and effectively. See full prescribing information for FLURBIPROFEN TABLETS. FLURBIPROFEN tablets, for oral use Initial U.S. Approval: 1988
7df104c9-edb9-6aaf-e053-2a91aa0aefad
HUMAN PRESCRIPTION DRUG LABEL
Feb 29, 2024
Medsource pharmaceuticals
DUNS: 833685915
Products 1
Detailed information about drug products covered under this FDA approval, including NDC codes, dosage forms, ingredients, and administration routes.
Flurbiprofen
Product Details
FDA regulatory identification and product classification information
FDA Identifiers
Product Classification
Product Specifications
INGREDIENTS (13)
Drug Labeling Information
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
Package/Label Display Panel - 60 count
BOXED WARNING SECTION
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
See full prescribing information for complete boxed warning.
*Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use (5.1) *Flurbiprofen tablets are contraindicated in the setting of coronary artery bypass graft (CABG) surgery (4,5.1) *NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events (5.2)
INDICATIONS & USAGE SECTION
1 INDICATIONS AND USAGE
Flurbiprofen tablets are indicated:
- For relief of the signs and symptoms of rheumatoid arthritis.
- For relief of the signs and symptoms of osteoarthritis.
Flurbiprofen tablets are a nonsteroidal anti-inflammatory drug indicated for (1)
- Relief of the signs and symptoms of rheumatoid arthritis
- Relief of the signs and symptoms of osteoarthritis
CONTRAINDICATIONS SECTION
4 CONTRAINDICATIONS
- Flurbiprofen tablets are contraindicated in the following patients:
- Known hypersensitivity (e.g., anaphylactic reactions and serious skin reactions) to flurbiprofen or any components of the drug product [ see Warnings and Precautions ( 5.7, 5.9) ]
- History of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs. Severe, sometimes fatal, anaphylactic reactions to nonsteroidal anti-inflammatory drugs have been reported in such patients [ see Warnings and Precautions ( 5.7, 5.8) ].
- In the setting of coronary artery bypass graft (CABG) surgery [ see Warnings and Precautions ( 5.1) ].
- Known hypersensitivity to flurbiprofen or any components of the drug product ( 5.7, 5.9)
- History of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs ( 5.7, 5.8)
- In the setting of CABG surgery ( 5.1)
ADVERSE REACTIONS SECTION
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling:
- Cardiovascular Thrombotic Events [ see Warnings and Precautions ( 5.1) ]
- GI Bleeding, Ulceration and Perforation [ see Warnings and Precautions ( 5.2) ]
- Hepatotoxicity [ see Warnings and Precautions ( 5.3) ]
- Hypertension [ see Warnings and Precautions ( 5.4) ]
- Heart Failure and Edema [ see Warnings and Precautions ( 5.5) ]
- Renal Toxicity and Hyperkalemia [ see Warnings and Precautions ( 5.6) ]
- Anaphylactic Reactions [ see Warnings and Precautions ( 5.7) ]
- Serious Skin Reactions [ see Warnings and Precautions ( 5.9) ]
- Hematologic Toxicity [ see Warnings and Precautions ( 5.11) ]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Incidence of 1% or greater
**Body as a whole:**edema
**Digestive system:**GI bleeding, abdominal pain, constipation, diarrhea,
dyspepsia/heartburn, flatulence, nausea, vomiting, elevated liver enzymes
**Metabolic and nutritional system:**body weight changes
**Nervous system:**headache, nervousness, anxiety, insomnia, increased
reflexes, tremor, amnesia, asthenia, depression, malaise, somnolence
**Respiratory system:**rhinitis
**Skin and appendages:**rash
**Special senses:**changes in vision, dizziness, tinnitus
**Urogenital system:**signs and symptoms suggesting urinary tract infection
Incidence < 1%
**Body as a whole:**anaphylactic reaction, chills, fever
**Cardiovascular system:myocardial infarction, congestive heart failure,
hypertension, vascular diseases, vasodilationDigestive
system:**gastric/peptic ulcer disease, hematemesis, bloody diarrhea,
hepatitis, esophageal disease, gastritis, stomatitis/glossitis, dry mouth
**Hemic and lymphatic system:**iron deficiency anemia, decrease in hemoglobin
and hematocrit, purpura, eosinophilia
**Metabolic and nutritional system:**hyperuricemia
**Nervous system:**cerebrovascular ischemia, convulsion, ataxia, confusion,
hypertonia, paresthesia, twitching, emotional lability
**Respiratory system:**asthma, dyspnea, epistaxis, bronchitis, laryngitis
**Skin and appendages:**angioedema, urticaria, eczema, pruritus, herpes
simplex, alopecia, dry skin
**Special senses:**vertigo, corneal opacity, parosmia, conjunctivitis
**Urogenital system:**renal failure, vaginal hemorrhage, hematuria
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of flurbiprofen. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
**Cardiovascular system:**angina pectoris, arrhythmias
**Digestive system:**jaundice (cholestatic and noncholestatic), colitis, small
intestine inflammation with loss of blood and protein, exacerbation of
inflammatory bowel disease, cholecystitis, periodontal abscess, appetite
changes
**Hemic and lymphatic system:**aplastic anemia (including agranulocytosis or
pancytopenia), hemolytic anemia, leukopenia, thrombocytopenia, ecchymosis,
lymphadenopathy
**Metabolic and nutritional system:**hyperkalemia
**Nervous system:**cerebrovascular accident, subarachnoid hemorrhage,
meningitis, myasthenia
**Respiratory system:**pulmonary infarct, pulmonary embolism,
hyperventilation,
**Skin and appendages:**toxic epidermal necrolysis, exfoliative dermatitis,
zoster, photosensitivity, nail disorder, sweating
**Special senses:**retinal hemorrhage, glaucoma, retrobulbar neuritis,
transient hearing loss, changes in taste, ear disease
**Urogenital system:**interstitial nephritis, uterine hemorrhage, menstrual
disturbances, prostate disease, vulvovaginitis
Most common adverse reactions (incidence > 3% from clinical trials) are: abdominal pain, dyspepsia, nausea, diarrhea, constipation, headache, edema, signs and symptoms suggesting urinary tract infection ( 6.1)
**To report SUSPECTED ADVERSE REACTIONS, contactTEVA USA, PHARMACOVIGILANCE at 1-866-832-8537or FDA at 1-800-FDA-1088 or **www.fda.gov/medwatch.
DRUG INTERACTIONS SECTION
7 DRUG INTERACTIONS
See Table 1 for clinically significant drug interactions with flurbiprofen.
Table 1: Clinically Significant Drug Interactions with Flurbiprofen|
Drugs That Interfere with Hemostasis | |
|
Clinical Impact: |
|
|
Intervention: |
Monitor patients with concomitant use of flurbiprofen with anticoagulants (e.g., warfarin), antiplatelet agents (e.g., aspirin), selective serotonin reuptake inhibitors (SSRIs), and serotonin norepinephrine reuptake inhibitors (SNRIs) for signs of bleeding [ see Warnings and Precautions ( 5) ]. |
|
Aspirin | |
|
Clinical Impact: |
Controlled clinical studies showed that the concomitant use of NSAIDs and analgesic doses of aspirin does not produce any greater therapeutic effect than the use of NSAIDs alone. In a clinical study, the concomitant use of an NSAID and aspirin was associated with a significantly increased incidence of GI adverse reactions as compared to use of the NSAID alone [ see Warnings and Precautions ( 5) ]. Concurrent administration of aspirin lowers serum flurbiprofen concentrations. The clinical significance of this interaction is not known. |
|
Intervention: |
Concomitant use of flurbiprofen and analgesic doses of aspirin is not generally recommended because of the increased risk of bleeding [ see Warnings and Precautions ( 5) ]. Flurbiprofen is not a substitute for low dose aspirin for cardiovascular protection. |
|
ACE Inhibitors, Angiotensin Receptor Blockers, and Beta-Blockers | |
|
Clinical Impact: |
|
|
Intervention: |
|
|
Diuretics | |
|
Clinical Impact: |
Clinical studies, as well as post-marketing observations, showed that NSAIDs reduced the natriuretic effect of loop diuretics (e.g., furosemide) and thiazide diuretics in some patients. This effect has been attributed to the NSAID inhibition of renal prostaglandin synthesis. |
|
Intervention: |
During concomitant use of flurbiprofen with diuretics, observe patients for signs of worsening renal function, in addition to assuring diuretic efficacy including antihypertensive effects [ see Warnings and Precautions ( 5) ]. |
|
Digoxin | |
|
Clinical Impact: |
The concomitant use of flurbiprofen with digoxin has been reported to increase the serum concentration and prolong the half-life of digoxin [ see Clinical Pharmacology ( 12.3) ]. |
|
Intervention: |
During concomitant use of flurbiprofen and digoxin, monitor serum digoxin levels. |
|
Lithium | |
|
Clinical Impact: |
NSAIDs have produced elevations in plasma lithium levels and reductions in renal lithium clearance .The mean minimum lithium concentration increased 15%, and the renal clearance decreased by approximately 20%. This effect has been attributed to NSAID inhibition of renal prostaglandin synthesis. |
|
Intervention: |
During concomitant use of flurbiprofen and lithium, monitor patients for signs of lithium toxicity. |
|
Methotrexate | |
|
Clinical Impact: |
Concomitant use of NSAIDs and methotrexate may increase the risk for methotrexate toxicity (e.g., neutropenia, thrombocytopenia, renal dysfunction). |
|
Intervention: |
During concomitant use of flurbiprofen and methotrexate, monitor patients for methotrexate toxicity. |
|
Cyclosporine | |
|
Clinical Impact: |
Concomitant use of flurbiprofen and cyclosporine may increase cyclosporine’s nephrotoxicity. |
|
Intervention: |
During concomitant use of flurbiprofen and cyclosporine, monitor patients for signs of worsening renal function. |
|
NSAIDs and Salicylates | |
|
Clinical Impact: |
Concomitant use of flurbiprofen with other NSAIDs or salicylates (e.g., diflunisal, salsalate) increases the risk of GI toxicity, with little or no increase in efficacy [ see Warnings and Precautions ( 5.2) ]. |
|
Intervention: |
The concomitant use of flurbiprofen with other NSAIDs or salicylates is not recommended. |
|
Pemetrexed | |
|
Clinical Impact: |
Concomitant use of flurbiprofen and pemetrexed may increase the risk of pemetrexed-associated myelosuppression, renal, and GI toxicity (see the pemetrexed prescribing information). |
|
Intervention: |
During concomitant use of flurbiprofen and pemetrexed, in patients with renal impairment whose creatinine clearance ranges from 45 to 79 mL/min, monitor for myelosuppression, renal and GI toxicity. NSAIDs with short elimination half-lives (e.g., diclofenac, indomethacin) should be avoided for a period of two days before, the day of, and two days following administration of pemetrexed. In the absence of data regarding potential interaction between pemetrexed and NSAIDs with longer half-lives (e.g., meloxicam, nabumetone), patients taking these NSAIDs should interrupt dosing for at least five days before, the day of, and two days following pemetrexed administration. |
|
Corticosteroids | |
|
Clinical Impact: |
Concomitant use of corticosteroids with flurbiprofen may increase the risk of GI ulceration or bleeding. |
|
Intervention: |
Monitor patients with concomitant use of flurbiprofen with corticosteroids for signs of bleeding [ see Warnings and Precautions ( 5.2) ]. |
- Drugs that Interfere with Hemostasis (e.g. warfarin, aspirin, SSRIs/SNRIs): Monitor patients for bleeding who are concomitantly taking flurbiprofen with drugs that interfere with hemostasis. Concomitant use of flurbiprofen and analgesic doses of aspirin is not generally recommended ( 7)
- ACE Inhibitors, Angiotensin Receptor Blockers (ARB), or Beta-Blockers: Concomitant use with flurbiprofen may diminish the antihypertensive effect of these drugs. Monitor blood pressure ( 7)
- ACE Inhibitors and ARBs: Concomitant use with flurbiprofen in elderly, volume depleted, or those with renal impairment may result in deterioration of renal function. In such high risk patients, monitor for signs of worsening renal function ( 7)
- Diuretics: NSAIDs can reduce natriuretic effect of furosemide and thiazide diuretics. Monitor patients to assure diuretic efficacy including antihypertensive effects ( 7)
RECENT MAJOR CHANGES SECTION
RECENT MAJOR CHANGES
|
Boxed Warning |
5/2016 |
|
Warnings and Precautions, Cardiovascular Thrombotic Events ( 5.1) |
5/2016 |
|
Warnings and Precautions, Heart Failure and Edema ( 5.5) |
5/2016 |
DOSAGE & ADMINISTRATION SECTION
2 DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of flurbiprofen tablets and other treatment options before deciding to use flurbiprofen tablets. Use the lowest effective dosage for the shortest duration consistent with individual patient treatment goals [ see Warnings and Precautions (5) ].
After observing the response to initial therapy with flurbiprofen tablets, the dose and frequency should be adjusted to suit an individual patient's needs.
For relief of the signs and symptoms of rheumatoid arthritis or osteoarthritis, the dosage is 200 to 300 mg per day, divided for administration two, three, or four times a day. The largest recommended single dose in a multiple-dose daily regimen is 100 mg.
- Use the lowest effective dosage for shortest duration consistent with individual patient treatment goals ( 2)
- The recommended starting dose of flurbiprofen tablets is 200 to 300 mg per day, divided for administration two, three, or four times a day. The largest recommended single dose in a multiple-dose daily regimen is 100 mg ( 2)
DOSAGE FORMS & STRENGTHS SECTION
3 DOSAGE FORMS AND STRENGTHS
Flurbiprofen tablets USP: 100 mg round, blue, film-coated tablets debossed “93”-“711”
Flurbiprofen tablet USP, 100 mg ( 3)
USE IN SPECIFIC POPULATIONS SECTION
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Use of NSAIDs, including flurbiprofen, during the third trimester of pregnancy
increases the risk of premature closure of the fetal ductus arteriosus. Avoid
use of NSAIDs, including flurbiprofen, in pregnant women starting at 30 weeks
of gestation (third trimester).
There are no adequate and well-controlled studies of flurbiprofen in pregnant women. Data from observational studies regarding potential embryo-fetal risks of NSAID use in women in the first or second trimesters of pregnancy are inconclusive. In the general U.S. population, all clinically recognized pregnancies, regardless of drug exposure, have a background rate of 2 to 4% for major malformations, and 15 to 20% for pregnancy loss. In animal reproduction studies, delayed parturition, prolonged labor, stillborn fetuses, and the presence of retained fetuses at necropsy occurred following treatment of pregnant rats treated with oral flurbiprofen throughout gestation until labor at less than 1-time the human dose of 300 mg/day. Embryofetal lethality was seen in pregnant rats and rabbits administered oral flurbiprofen during the period of organogenesis at exposures 0.03-times and 0.5 times, respectively, the human dose of 300 mg. No evidence of malformations were noted in rats, rabbits, or mice treated with flurbiprofen during the period of organogenesis at doses that were 0.8-, 0.5-, and 0.2-times the maximum human daily dose [see Data]. Based on animal data, prostaglandins have been shown to have an important role in endometrial vascular permeability, blastocyst implantation, and decidualization. In animal studies, administration of prostaglandin synthesis inhibitors such as flurbiprofen, resulted in increased pre- and post-implantation loss.
Clinical Considerations
Labor or Delivery
There are no studies on the effects of flurbiprofen during labor or delivery.
In animal studies, NSAIDS, including flurbiprofen, inhibit prostaglandin
synthesis, cause delayed parturition, and increase the incidence of
stillbirth.
Data
Animal data
Pregnant rats were treated with oral doses of 0.05, 1, and 3 mg/kg
flurbiprofen 14 days prior to mating through Gestation Day (GD) 16.
Embryofetal lethality was seen at 1 mg/kg and above (0.03 times the maximum
recommended human dose [MRHD] of 300 mg on a mg/m 2basis). No maternal
toxicity was evident at this dose. No malformations were seen in fetuses from
pregnant rats administered flurbiprofen during the period of organogenesis at
doses up to 25 mg/kg (0.8 times the MRHD on a mg/m 2basis). Maternal toxicity
(uterine hemorrhage, gastric ulcers) was observed at this dose.
Pregnant rabbits were administered oral doses of 0.675, 2.25, and 7.5 mg/kg flurbiprofen from GD 1 through GD 29. Embryofetal lethality, but no evidence of teratogenicity, was seen at 7.5 mg/kg (0.5 times the MRHD of 300 mg on a mg/m 2basis). Maternal toxicity (gastric ulcers and lethality) was observed at this dose.
Pregnant mice were treated with oral doses of 2, 5, and 12 mg/kg flurbiprofen from GD 3 to 18. An increased incidence of fetal lethality occurred in the 12 mg/kg group (0.2 times the MRHD). All doses were associated with some evidence of maternal toxicity (placental hemorrhage).
Pregnant rats were treated with oral doses of 0.2, 0.675, 2.25, 7.5, and 25 mg/kg flurbiprofen from GD 1 until labor. Delayed delivery, the incidence of stillborn pups, and decreased pup viability, were noted at doses of 2.25 mg/kg and higher (0.07 times the MRHD). These doses were associated with maternal toxicity (uterine hemorrhage, gastrointestinal ulceration, decreased body weight).
Pregnant rats treated with oral doses of 0.4, 4, and 10 mg/kg flurbiprofen from GD 16 to labor, delayed parturition was seen at 0.4 mg/kg and above and stillborn pups were seen at 4 mg/kg and above (0.01-times and 0.13 times, respectively, the MRHD on mg/m 2basis). Uterine hemorrhage, ulceration, and mortality were noted in dams at 0.4 mg/kg and above.
8.2 Lactation
Risk Summary
Flurbiprofen is poorly excreted into human milk. The nursing infant dose is
predicted to be approximately 0.1 mg/day in the established milk of a woman
taking flurbiprofen 200 mg/day. The developmental and health benefits of
breastfeeding should be considered along with the mother’s clinical need for
flurbiprofen and any potential adverse effects on the breastfed infant from
flurbiprofen or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
Infertility
Females
Based on the mechanism of action, the use of prostaglandin-mediated NSAIDs,
including flurbiprofen, may delay or prevent rupture of ovarian follicles,
which has been associated with reversible infertility in some women. Published
animal studies have shown that administration of prostaglandin synthesis
inhibitors has the potential to disrupt prostaglandin-mediated follicular
rupture required for ovulation. Small studies in women treated with NSAIDs
have also shown a reversible delay in ovulation. Consider withdrawal of
NSAIDs, including flurbiprofen, in women who have difficulties conceiving or
who are undergoing investigation of infertility.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
Elderly patients, compared to younger patients, are at greater risk for NSAID- associated serious cardiovascular, gastrointestinal, and/or renal adverse reactions. If the anticipated benefit for the elderly patient outweighs these potential risks, start dosing at the low end of the dosing range, and monitor patients for adverse effects [ see Warnings and Precautions ( 5.1, 5.2, 5.3, 5.6, 5.13) ].
Pregnancy: Use of NSAIDs during the third trimester of pregnancy increases the risk of premature closure of the fetal ductus arteriosus. Avoid use of NSAIDs in pregnant women starting at 30 weeks gestation ( 5.10, 8.1)
Infertility: NSAIDs are associated with reversible infertility. Consider withdrawal of flurbiprofen in women who have difficulties conceiving ( 8.3)
DESCRIPTION SECTION
11 DESCRIPTION
Flurbiprofen tablets USP are a member of the phenylalkanoic acid derivative group of nonsteroidal anti-inflammatory drug. Flurbiprofen tablets USP are round, blue, film-coated debossed “93” – “711” tablets for oral administration. Flurbiprofen, USP is a racemic mixture of (+)S- and (-)R- enantiomers. Flurbiprofen, USP is a white or slightly yellow crystalline powder. It is slightly soluble in water at pH 7.0 and readily soluble in most polar solvents. The chemical name is [1,1’-biphenyl]-4-acetic acid,2-fluoro-α- methyl-, (±)-. It has the following structural formula:
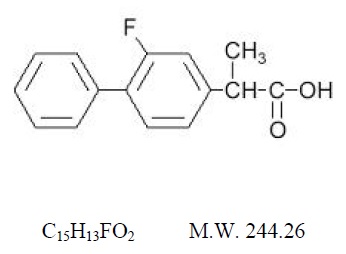
Each tablet, for oral administration, contains 100 mg flurbiprofen, USP. In addition, each tablet contains the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate 80, titanium dioxide, and FD&C Blue #1 aluminum lake.
CLINICAL PHARMACOLOGY SECTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Flurbiprofen has analgesic, anti-inflammatory, and antipyretic properties.
The mechanism of action of flurbiprofen, like that of other NSAIDs, is not completely understood but involves inhibition of cyclooxygenase (COX-1 and COX-2).
Flurbiprofen is a potent inhibitor of prostaglandin (PG) synthesis in vitro. Flurbiprofen concentrations reached during therapy have produced in vivo effects. Prostaglandins sensitize afferent nerves and potentiate the action of bradykinin in inducing pain in animal models. Prostaglandins are mediators of inflammation. Because flurbiprofen is an inhibitor of prostaglandin synthesis, its mode of action may be due to a decrease of prostaglandins in peripheral tissues.
12.3 Pharmacokinetics
General pharmacokinetic characteristics
The pharmacokinetics of flurbiprofen have been characterized in healthy
subjects, special populations and patients (see Table 2). The pharmacokinetics
of flurbiprofen are linear, and there is little accumulation of flurbiprofen
following multiple doses of flurbiprofen.
Þ | ||||
|
Pharmacokinetic Parameter |
Normal Healthy Adults***** |
Geriatric Arthritis Patients†**** |
End Stage Renal Disease Patients***** |
Alcoholic Cirrhosis Patients‡ (31 to 61 years) N = 8 |
|
Peak Concentration (mcg/mL) |
14 (4) |
16 (5) |
9 § |
9 § |
|
Time to Reach Peak Concentration (h) |
1.9 (1.5) |
2.2 (3) |
2.3 § |
1.2 § |
|
Urinary Recovery of Unchanged Flurbiprofen (% of Dose) |
2.9 (1.3) |
0.6 (0.6) |
0.02 (0.02) |
NA ¶ |
|
Area Under the Curve (AUC) |
83 (20) |
77 (24) |
44 § |
50 § |
|
Apparent Volume of Distribution (Vz/F, L) |
14 (3) |
12 (5) |
10 § |
14 § |
|
Terminal Elimination Half-life |
7.5 (0.8) |
5.8 (1.9) |
3.3 Þ |
5.4 Þ |
Absorption
The mean oral bioavailability of flurbiprofen from flurbiprofen tablets 100 mg
is 96% relative to an oral solution. Flurbiprofen is rapidly and non-
stereoselectively absorbed from flurbiprofen, with peak plasma concentrations
occurring at approximately 2 hours (see Table 2).
Administration of flurbiprofen with either food or antacids may alter the rate but not the extent of flurbiprofen absorption. Ranitidine has been shown to have no effect on either the rate or extent of flurbiprofen absorption from flurbiprofen.
Distribution
The apparent volume of distribution (Vz/F) of both R- and S-flurbiprofen is
approximately 0.12 L/kg. Both flurbiprofen enantiomers are more than 99% bound
to plasma proteins, primarily albumin. Plasma protein binding is relatively
constant for the typical average steady-state concentrations (≤ 10 mcg/mL)
achieved with recommended doses. Flurbiprofen is poorly excreted into human
milk. The nursing infant dose is predicted to be approximately 0.1 mg/day in
the established milk of a woman taking flurbiprofen 200 mg/day.
Metabolism
Several flurbiprofen metabolites have been identified in human plasma and
urine. These metabolites include 4’-hydroxy-flurbiprofen, 3’, 4’-dihydroxy-
flurbiprofen, 3’-hydroxy-4’-methoxy-flurbiprofen, their conjugates, and
conjugated flurbiprofen. Unlike other arylpropionic acid derivatives (e.g.,
ibuprofen), metabolism of R-flurbiprofen to S-flurbiprofen is minimal.
In vitrostudies have demonstrated that cytochrome CYP2C9 plays an important role in the metabolism of flurbiprofen to its major metabolite 4’-hydroxy- flurbiprofen. The 4’-hydroxy-flurbiprofen metabolite showed little anti- inflammatory activity in animal models of inflammation. In vitrostudies also demonstrated glucuronidation of both enantiomers of flurbiprofen and 4’-hydroxy-flurbiprofen. UGT2B7 is the predominant UGT isozyme responsible for the glucuronidation. Flurbiprofen does not induce enzymes that alter its metabolism.
Excretion
Following dosing with flurbiprofen, less than 3% of flurbiprofen is excreted
unchanged in the urine, with about 70% of the dose eliminated in the urine as
flurbiprofen, 4’-hydroxy-flurbiprofen, and their acylglucuronide conjugates.
Because renal elimination is a significant pathway of elimination of
flurbiprofen metabolites, dosing adjustment in patients with moderate or
severe renal dysfunction may be necessary to avoid accumulation of
flurbiprofen metabolites.
The mean terminal elimination half-lives (t ½) of R- and S-flurbiprofen are similar, about 4.7 and 5.7 hours, respectively.
Specific Populations
Pediatric:The pharmacokinetics of flurbiprofen have not been investigated in
pediatric patients.
Race:No pharmacokinetic differences due to race have been identified.
Geriatric:Flurbiprofen pharmacokinetics were similar in geriatric arthritis patients, younger arthritis patients, and young healthy volunteers receiving flurbiprofen 100 mg as either single or multiple doses.
Hepatic Impairment:Hepatic metabolism may account for > 90% of flurbiprofen elimination, so patients with hepatic disease may require reduced doses of flurbiprofen compared to patients with normal hepatic function. The pharmacokinetics of R- and S-flurbiprofen were similar, however, in alcoholic cirrhosis patients (N = 8) and young healthy volunteers (N = 8) following administration of a single 200 mg dose of flurbiprofen. Flurbiprofen plasma protein binding may be decreased in patients with liver disease and serum albumin concentrations below 3.1 g/dL.
Renal Impairment:Renal clearance is an important route of elimination for flurbiprofen metabolites, but a minor route of elimination for unchanged flurbiprofen (≤ 3% of total clearance). The unbound clearances of R- and S-flurbiprofen did not differ significantly between normal healthy volunteers (N = 6, 50 mg single dose) and patients with renal impairment (N = 8, inulin clearances ranging from 11 to 43 mL/min, 50 mg multiple doses). Flurbiprofen plasma protein binding may be decreased in patients with renal impairment and serum albumin concentrations below 3.9 g/dL. Elimination of flurbiprofen metabolites may be reduced in patients with renal impairment.
Flurbiprofen is not significantly removed from the blood into dialysate in patients undergoing continuous ambulatory peritoneal dialysis.
Drug Interaction Studies
Antacids:
Administration of flurbiprofen to volunteers under fasting conditions or with
antacid suspension yielded similar serum flurbiprofen-time profiles in young
adult subjects (n = 12). In geriatric subjects (n = 7), there was a reduction
in the rate but not the extent of flurbiprofen absorption.
Aspirin:
Concurrent administration of flurbiprofen and aspirin resulted in 50% lower
serum flurbiprofen concentrations. This effect of aspirin (which is also seen
with other NSAIDs) has been demonstrated in patients with rheumatoid arthritis
(n = 15) and in healthy volunteers (n = 16) [ see Drug Interactions ( 7) ].
Beta-adrenergic Blocking Agents:
The effect of flurbiprofen on blood pressure response to propranolol and
atenolol was evaluated in men with mild uncomplicated hypertension (n = 10).
Flurbiprofen pretreatment attenuated the hypotensive effect of a single dose
of propranolol but not atenolol. Flurbiprofen did not appear to affect the
beta-blocker-mediated reduction in heart rate. Flurbiprofen did not affect the
pharmacokinetic profile of either drug [ see Drug Interactions ( 7) ].
Cimetidine, Ranitidine:
In normal volunteers (n = 9), pretreatment with cimetidine or ranitidine did
not affect flurbiprofen pharmacokinetics, except for a small (13%) but
statistically significant increase in the area under the serum concentration
curve of flurbiprofen in subjects who received cimetidine.
Digoxin:
In studies of healthy males (n = 14), concomitant administration of
flurbiprofen and digoxin did not change the steady state serum levels of
either drug [ see Drug Interactions ( 7) ].
Diuretics:
Studies in healthy volunteers have shown that, like other NSAIDs, flurbiprofen
can interfere with the effects of furosemide. Although results have varied
from study to study, effects have been shown on furosemide-stimulated
diuresis, natriuresis, and kaliuresis [ see Drug Interactions ( 7) ].
Lithium:
In a study of 11 women with bipolar disorder receiving lithium carbonate at a
dosage of 600 to 1200 mg/day, administration of 100 mg flurbiprofen every 12
hours increased plasma lithium concentrations by 19%. Four of 11 patients
experienced a clinically important increase (> 25% or > 0.2 mmol/L) [ see Drug Interactions ( 7) ].
Methotrexate:
In a study of six adult arthritis patients, coadministration of methotrexate
(10 to 25 mg/dose) and flurbiprofen (300 mg/day) resulted in no observable
interaction between these two drugs [ see Drug Interactions ( 7) ].
Oral Hypoglycemic Agents:
In a clinical study, flurbiprofen was administered to adult diabetics who were
already receiving glyburide (n = 4), metformin (n = 2), chlorpropamide with
phenformin (n=3), or glyburide with phenformin (n = 6). Although there was a
slight reduction in blood sugar concentrations during concomitant
administration of flurbiprofen and hypoglycemic agents, there were no signs or
symptoms of hypoglycemia.
Poor Metabolizers of CYP2C9 Substrates:
In patients who are known or suspected to be poor CYP2C9 metabolizers based on
genotype or previous history/experience with other CYP2C9 substrates (such as
warfarin and phenytoin), reduce the dose of flurbiprofen to avoid abnormally
high plasma levels due to reduced metabolic clearance.
HOW SUPPLIED SECTION
16 HOW SUPPLIED/STORAGE AND HANDLING
Flurbiprofen tablets USP, 100 mg are round, blue, film-coated tablets debossed “93”-“711” available in bottles of 100 (NDC 0093-0711-01) and 500 (NDC 0093-0711-05).
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
SPL MEDGUIDE SECTION
MEDICATION GUIDE
|
Medication Guide for Nonsteroidal Anti-inflammatory Drugs (NSAIDs)****. |
|
What is the most important information I should know about medicines called Nonsteroidal Anti-inflammatory Drugs (NSAIDs)? NSAIDs can cause serious side effects, including: ***Increased risk of a heart attack or stroke that can lead to death.**This risk may happen early in treatment and may increase:
Do not take NSAIDs right before or after a heart surgery called a “coronary artery bypass graft (CABG).” Avoid taking NSAIDs after a recent heart attack, unless your healthcare provider tells you to. You may have an increased risk of another heart attack if you take NSAIDs after a recent heart attack. *Increased risk of bleeding, ulcers, and tears (perforation) of the esophagus (tube leading from the mouth to the stomach), stomach and intestines: * anytime during use * without warning symptoms * that may cause death The risk of getting an ulcer or bleeding increases with:
NSAIDs should only be used:
|
|
What are NSAIDs? NSAIDs are used to treat pain and redness, swelling, and heat (inflammation) from medical conditions such as different types of arthritis, menstrual cramps, and other types of short-term pain. |
|
Who should not take NSAIDs? Do not take NSAIDs:
|
|
Before taking NSAIDs, tell your healthcare provider about all of your medical conditions, including if you:
**Tell your healthcare provider about all of the medicines you take, including prescription or over-the-counter medicines, vitamins or herbal supplements.**NSAIDs and some other medicines can interact with each other and cause serious side effects.Do not start taking any new medicine without talking to your healthcare provider first. |
|
What are the possible side effects of NSAIDs? NSAIDs can cause serious side effects, including: See “What is the most important information I should know about medicines called Nonsteroidal Anti-inflammatory Drugs (NSAIDs)?
Get emergency help right away if you get any of the following symptoms:
Stop taking your NSAID and call your healthcare provider right away if you get any of the following symptoms:
If you take too much of your NSAID, call your healthcare provider or get medical help right away. These are not all the possible side effects of NSAIDs. For more information, ask your healthcare provider or pharmacist about NSAIDs. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
Other information about NSAIDs
|
|
General information about the safe and effective use of NSAIDs Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use NSAIDs for a condition for which it was not prescribed. Do not give NSAIDs to other people, even if they have the same symptoms that you have. It may harm them. If you would like more information about NSAIDs, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about NSAIDs that is written for health professionals. |
|
This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised May 2016 |
INFORMATION FOR PATIENTS SECTION
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide) that accompanies each prescription dispensed. Inform patients, families, or their caregivers of the following information before initiating therapy with flurbiprofen and periodically during the course of ongoing therapy.
Cardiovascular Thrombotic Events
Advise patients to be alert for the symptoms of cardiovascular thrombotic
events, including chest pain, shortness of breath, weakness, or slurring of
speech, and to report any of these symptoms to their health care provider
immediately [ see Warnings and Precautions ( 5) ].
Gastrointestinal Bleeding, Ulceration, and Perforation
Advise patients to report symptoms of ulcerations and bleeding, including
epigastric pain, dyspepsia, melena, and hematemesis to their health care
provider. In the setting of concomitant use of low-dose aspirin for cardiac
prophylaxis, inform patients of the increased risk for and the signs and
symptoms of GI bleeding [ see Warnings and Precautions ( 5) ].
Hepatotoxicity
Inform patients of the warning signs and symptoms of hepatotoxicity (e.g.,
nausea, fatigue, lethargy, pruritus, diarrhea, jaundice, right upper quadrant
tenderness, and “flu-like” symptoms). If these occur, instruct patients to
stop flurbiprofen and seek immediate medical therapy [ see Warnings and Precautions ( 5) ].
Heart Failure and Edema
Advise patients to be alert for the symptoms of congestive heart failure
including shortness of breath, unexplained weight gain, or edema and to
contact their healthcare provider if such symptoms occur [ see Warnings and Precautions ( 5) ].
Anaphylactic Reactions
Inform patients of the signs of an anaphylactic reaction (e.g., difficulty
breathing, swelling of the face or throat). Instruct patients to seek
immediate emergency help if these occur [ see Contraindications ( 4) and Warnings and Precautions ( 5) ].
Serious Skin Reactions
Advise patients to stop flurbiprofen immediately if they develop any type of
rash and to contact their healthcare provider as soon as possible [ see Warnings and Precautions ( 5) ].
Female Fertility
Advise females of reproductive potential who desire pregnancy that NSAIDs,
including flurbiprofen, may be associated with a reversible delay in ovulation
[ see Use in Specific Populations ( 8.3) ].
Fetal Toxicity
Inform pregnant women to avoid use of flurbiprofen and other NSAIDs starting
at 30 weeks gestation because of the risk of the premature closing of the
fetal ductus arteriosus [ see Warnings and Precautions ( 5) and Use in Specific Populations ( 8) ].
Avoid Concomitant Use of NSAIDs
Inform patients that the concomitant use of flurbiprofen with other NSAIDs or
salicylates (e.g., diflunisal, salsalate) is not recommended due to the
increased risk of gastrointestinal toxicity, and little or no increase in
efficacy [ see Warnings and Precautions ( 5) and Drug Interactions ( 7) ].
Alert patients that NSAIDs may be present in “over the counter” medications
for treatment of colds, fever, or insomnia.
Use of NSAIDS and Low-Dose Aspirin
Inform patients not to use low-dose aspirin concomitantly with flurbiprofen
until they talk to their healthcare provider [ see Drug Interactions ( 7) ].
Manufactured In India By:
PIRAMAL ENTERPRISES LIMITED
Pithampur, Madhya Pradesh, India
Manufactured For:
TEVA****PHARMACEUTICALS USA, INC.
North Wales, PA 19454
Rev. K 5/2016
OVERDOSAGE SECTION
10 OVERDOSAGE
Symptoms following acute NSAID overdosages have been typically limited to lethargy, drowsiness, nausea, vomiting, and epigastric pain, which are generally reversible with supportive care. Gastrointestinal bleeding has occurred. Hypertension, acute renal failure, respiratory depression and coma have occurred, but were rare [ see Warnings and Precautions ( 5.1, 5.2, 5.4, 5.6) ].
Manage patients with symptomatic and supportive care following an NSAID overdosage. There are no specific antidotes. Consider emesis and/or activated charcoal (60 to 100 grams in adults, 1 to 2 grams per kg of body weight in pediatric patients) and/or osmotic cathartic in symptomatic patients seen within four hours of ingestion or in patients with a large overdosage (5 to 10 times the recommended dosage). Forced diuresis, alkalinization of urine, hemodialysis, or hemoperfusion may not be useful due to high protein binding.
For additional information about overdosage treatment contact a poison control center (1-800-222-1222).
NONCLINICAL TOXICOLOGY SECTION
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Flurbiprofen was not carcinogenic in long-term studies in Fischer-344 and CD
rats at doses up to 5 mg/kg/day and in CFLP mice at doses up to 12 mg/kg/day
(0.16-times and 0.19-times, respectively, the human dose of 300 mg/day on a
mg/m 2basis).
Mutagenesis
Flurbiprofen was not genotoxic in an in vivomicronucleus assay in rats.
Impairment of Fertility
No effect on male or female fertility in rats was observed after oral
administration of 3 mg/kg flurbiprofen for 65 days prior to mating in males
and 14 days prior to mating through Gestation Day 16 in females (equivalent to
0.1-times the human dose of 300 mg/day on a mg/m 2basis). This dose was not
associated with significant toxicity in the dams or sires.