- Approval Id
- 10999b337de6053d
- Drug Name
- FONKOPAC CONCENTRATE FOR SOLUTION FOR INFUSION 6MG/ML
- Product Name
- FONKOPAC CONCENTRATE FOR SOLUTION FOR INFUSION 6MG/ML
- Approval Number
- SIN16410P
- Approval Date
- 2021-12-30
- Registrant
- GLORIOUS DEXA SINGAPORE PTE. LTD.
- Licence Holder
- GLORIOUS DEXA SINGAPORE PTE. LTD.
- Drug Type
- Therapeutic
- Forensic Classification
- Prescription Only
- Dosage Form
- INFUSION, SOLUTION CONCENTRATE
- Dosage
- **Dosage and administration:**
**Dosage**
Premedication
All patients must be given premedication prior to paclitaxel administration to reduce the risk of severe hypersensitivity reactions. Premedication is consisting of corticosteroids, antihistamines and H2-receptor antagonists prior to paclitaxel therapy.

Repeat courses of paclitaxel should not be administered to patients with solid tumors until the neutrophil count is at least 1500 cells/mm3 and the platelet count is at least 100,000 cells/mm3 (<1000 cells/mm3 for patients with Kaposi’s sarcoma). Patients who experience severe neutropenia (<500 cells/mm3) or severe peripheral neuropathy should receive a dosage reduced by 20% for subsequent courses. The incidence of neurotoxicity and the severity of neutropenia increase with dose within a regimen.
Metastatic carcinoma of the ovary:
_Combination therapy:_ For previously untreated patients, the recommended dosing regimen, given every 3 weeks, is paclitaxel administered intravenously over 3 hours at a dose of 175 mg/m2 followed by a platinum compound.
Alternatively, a more myelosuppressive regimen of paclitaxel may also be administered intravenously at a dose of 135 mg/m2 over 24 hours followed by a platinum compound, every 3 weeks.
_Single-agent therapy:_ In patients previously treated with chemotherapy the recommended regimen is 175 mg/m2 administered intravenously over 3 hours every 3 weeks.
Carcinoma of the breast
_Adjuvant therapy:_ paclitaxel 175 mg/m2 administered intravenously over 3 hours every 3 weeks for 4 courses sequentially to standard combination therapy.
_Single-agent, first-line therapy after relapse within 6 months of adjuvant therapy:_ paclitaxel 175 mg/m2 administered intravenously over 3 hours every 3 weeks.
_Combination, first-line therapy of advanced or metastatic breast cancer:_ in combination with trastuzumab, the recommended dose of paclitaxel is 175 mg/m2 administered intravenously over a period of 3 hours, with a 3-week interval between courses. Paclitaxel infusion may be started at the day following the first dose of trastuzumab or immediately after the subsequent doses of trastuzumab if the preceding dose of trastuzumab was well tolerated.
_Combination, first-line therapy of metastatic breast cancer:_ in combination with doxorubicin (50 mg/m2), paclitaxel should be administered 24 hours after doxorubicin. The recommended dose of paclitaxel is 220 mg/m2 administered intravenously over a period of 3 hours, with a 3-week interval between courses.
_Single-agent second-line therapy after failure of combination chemotherapy for metastatic disease:_ paclitaxel 175 mg/m2 administered intravenously over 3 hours every 3 weeks.
Non-small cell lung cancer carcinoma
_Combination therapy:_ for previously untreated patients, the recommended dosing regimen, given with a 3-week interval between courses, is paclitaxel 175 mg/m2 administered intravenously over 3 hours followed by a platinum compound.
Alternatively, a more myelosuppressive regimen of paclitaxel may be administered intravenously 135 mg/m2 over 24 hours followed by a platinum compound, with a 3-week interval between courses.
_Single-agent therapy:_ paclitaxel 175 to 225 mg/m2 administered intravenously over 3 hours every 3 weeks.
AIDS-related Kaposi’s sarcoma:
_Second-line therapy:_ paclitaxel 135 mg/m2 administered intravenously over 3 hours with a 3-week interval between courses or 100 mg/m2 administered intravenously over 3 hours with a 2-week interval between courses (dose intensity 45–50 mg/m2/week).
Based upon the immunosuppression observed in patients with advanced HIV disease, the following modifications are recommended in these patients.
1. The dose of dexamethasone as one of the three premedication drugs should be reduced to 10 mg orally.
2. Treatment with paclitaxel should be initiated or repeated only if the neutrophil count is at least 1000 cells/mm3.
3. The dose of subsequent courses of paclitaxel should be reduced by 20% for those patients who experience severe neutropenia (<500 cells/mm3 for a week or longer).
4. Concomitant hematopoietic growth factor (G-CSF), should be initiated as clinically indicated.
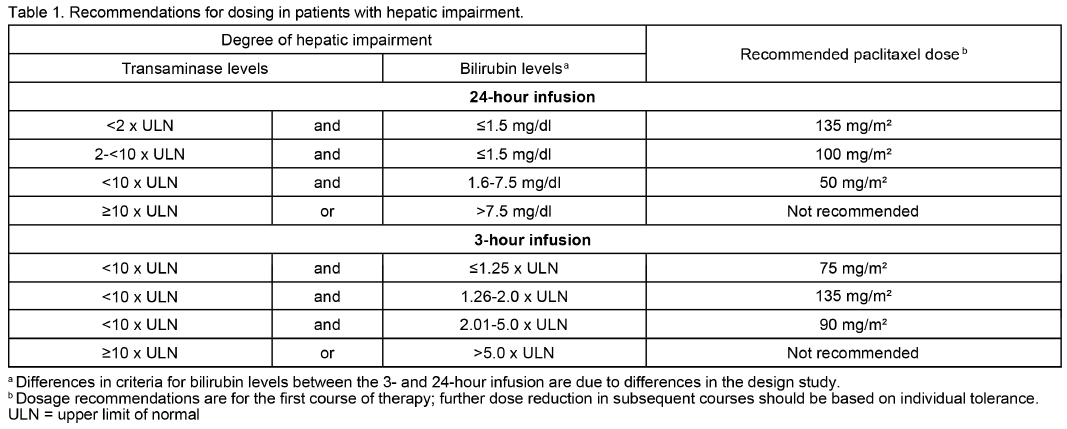
Hepatic impairment
Patients with hepatic impairment may be at increased risk of toxicity, particularly grade III–IV myelosuppression. Dose adjustment is recommended, as shown in Table 1 for both 3- and 24-hour infusions. Patients should be monitored closely for the development of profound myelosuppression.
**Administration**
Instructions for use, handling and disposal
Paclitaxel is a cytotoxic anticancer drug and caution should be exercised in handling paclitaxel. Dilution of paclitaxel should take place in designated area under aseptic conditions and be carried out by specially trained medical staff. The use of gloves is recommended.
If paclitaxel solution contacts the skin, wash the skin immediately and thoroughly with soap and water. If paclitaxel contacts mucous membranes, the membranes should be flushed thoroughly with water. Following topical exposure, events have included tingling, burning and redness. Upon inhalation, dyspnea, chest pain, burning eyes, sore throat and nausea have been reported. Given the possibility of extravasation, it is advisable to closely monitor the infusion site for possible infiltration during drug administration.
Paclitaxel should be administered through an in-line filter with a microporous membrane not greater than 0.22 microns. Use of filter devices which incorporate short inlet and outlet PVC-coated tubing has not resulted in significant leaching of di-(2-ethoxyhexyl) phthalate (DEHP).
Prior to infusion, FONKOPAC must be diluted under aseptic conditions in 0.9% sodium chloride injection or 5% glucose injection up to a final concentration of 0.3 mg/ml.
Upon preparation, solutions may show haziness, which is attributed to the formulation vehicle. No significant efficiency losses in potency have been noted following delivery of the solution through intravenous tubing containing an in-line 0.22 micron filter.
Paclitaxel solutions should be prepared and stored in glass containers. Non-PVC containing administration sets should be used.
Diluted solutions are chemically and physically stable for up to 48 hours at room temperature (approximately 25°C) and room lighting conditions; infusions should be completed within this time frame. Excessive agitation, vibration or shaking may induce precipitation and should be avoided. Infusion sets should be flushed thoroughly with a compatible diluent before use.
Devices with spikes should not be used with vials of paclitaxel since they can cause the stopper to collapse resulting in loss of sterile integrity of the paclitaxel solution.
Procedures for proper handling and disposal of anticancer drugs should be considered.
To minimize the risk of dermal exposure, always wear impervious gloves when handling vials containing paclitaxel. This includes all handling activities in clinical settings, pharmacies, store rooms, and home healthcare settings, including during unpacking and inspection, transport within a facility, and dose preparation and administration.
- Route Of Administration
- INTRAVENOUS
- Indication Info
- **Indications:**
**Ovarian carcinoma**
- First-line therapy in combination with a platinum compound for the treatment of advanced metastatic carcinoma of the ovary.
- Second-line therapy for the treatment of advanced metastatic carcinoma of the ovary.
**Breast carcinoma**
- Adjuvant treatment of node-positive breast cancer administered sequentially to standard combination therapy.
- First-line therapy of advanced or metastatic breast cancer after relapse within 6 months of adjuvant therapy. Prior therapy should have included an anthracycline unless clinically contraindicated.
- First-line therapy of metastatic breast cancer in combination with trastuzumab in patients who over-express HER-2 as determined by immunohistochemistry.
- First-line therapy of metastatic breast cancer in combination with an anthracycline in patients for whom anthracycline therapy is suitable.
- Second-line therapy of advanced or metastatic breast cancer after failure of combination chemotherapy for metastatic disease. Prior therapy should have included an anthracycline unless clinically contraindicated.
**Non-small cell lung carcinoma**
First-line therapy in combination with a platinum compound or as a single agent for the treatment of non-small cell carcinoma of the lung in patients who are not candidates for potentially curative surgery and/or radiation therapy.
**Kaposi’s sarcoma**
Second-line treatment of AIDS-related Kaposi’s sarcoma.
- Contraindications
- **Contraindications:**
- Patients who have a history of severe hypersensitivity reactions to paclitaxel or macrogolglycerol ricinoleate (polyoxyl castor oil) or to any of the excipients.
- Paclitaxel should not be administered to patients with solid tumors who have baseline neutrophil counts of <1500 cells/mm3 or patients with AIDS-related Kaposi’s sarcoma with baseline or subsequent neutrophil counts of <1000 cells/mm3.
- Atc Code
- L01CD01
- Atc Item Name
- paclitaxel
- Pharma Manufacturer Name
- GLORIOUS DEXA SINGAPORE PTE. LTD.
- Company Detail Path
- /organization/2aea0381f6373713/glorious-dexa-singapore-pte-ltd