
Regulatory Information
HSA regulatory responsibility and product classification details
Regulatory Responsibility
Product Classification
Formulation Information
CAPSULE
**4.2 Posology and method of administration** The daily dose of fluconazole should be based on the nature and severity of the fungal infection. Most cases of vaginal candidiasis respond to single-dose therapy. Therapy for those types of infections requiring multiple-dose treatment should be continued until clinical parameters or laboratory tests indicate that active fungal infection has subsided. An inadequate period of treatment may lead to recurrence of active infection. Patients with AIDS and cryptococcal meningitis or recurrent oropharyngeal candidiasis usually require maintenance therapy to prevent relapse. IN THE DOSING INSTRUCTIONS BELOW, THE DAILY DOSE OF FLUCONAZOLE IS THE SAME FOR ORAL (CAPSULES AND SUSPENSION) AND INTRAVENOUS ADMINISTRATION SINCE ORAL ABSORPTION IS RAPID AND ALMOST COMPLETE. Use in Adults 1. For cryptococcal meningitis and cryptococcal infections at other sites, the usual dose is 400 mg on the first day followed by 200 mg to 400 mg once daily. Duration of treatment for cryptococcal infections will depend on the clinical and mycological response, but is usually at least 6 to 8 weeks for cryptococcal meningitis. For the prevention of relapse of cryptococcal meningitis in patients with AIDS, after the patient receives a full course of primary therapy, fluconazole may be administered indefinitely at a once daily dose of 200 mg. 2. For candidemia, disseminated candidiasis and other invasive candidal infections, the usual dose is 400 mg on the first day followed by 200 mg once daily. Depending on the clinical response, the dose may be increased to 400 mg once daily. Duration of treatment is based upon the clinical response. 3. For oropharyngeal candidiasis, the usual dose is 50 mg to 100 mg once daily for 7 to 14 days. If necessary, treatment can be continued for longer periods in patients with severely compromised immune function. For atrophic oral candidiasis associated with dentures, the usual dose is 50 mg once daily for 14 days administered concurrently with local antiseptic measures to the denture. For other candidal infections of mucosa except genital candidiasis (see below) (e.g., esophagitis, non-invasive bronchopulmonary infections, candiduria, mucocutaneous candidiasis, etc.), the usual effective dose is 50 mg to 100 mg once daily, given for 14 to 30 days. 4. For the treatment of vaginal candidiasis, fluconazole 150 mg should be administered as a single oral dose. 5. The recommended fluconazole dosage for the prevention of candidiasis is 50 mg to 400 mg once daily, based on the patient’s risk for developing fungal infection. For patients at high risk of systemic infection, e.g., patients who are anticipated to have profound or prolonged neutropenia, the recommended daily dose is 400 mg once daily. Fluconazole administration should start several days before the anticipated onset of neutropenia and continue for 7 days after the neutrophil count rises above 1000 cells/mm3. 6. For dermal infections including tinea pedis, tinea corporis, tinea cruris and _Candida_ infections, the recommended dosage is 150 mg once weekly or 50 mg once daily. Duration of treatment is normally 2 to 4 weeks, but tinea pedis may require treatment for up to 6 weeks. Use in Children As with similar infections in adults, the duration of treatment is based on the clinical and mycological response. The maximum adult daily dosage should not be exceeded in children. Fluconazole is administered as a single dose each day. The recommended dosage of fluconazole for mucosal candidiasis is 3 mg/kg once daily. A loading dose of 6 mg/kg may be used on the first day to achieve steady-state levels more rapidly. For the treatment of systemic candidiasis and cryptococcal infections, the recommended dosage is 6 to 12 mg/kg once daily, depending on the severity of the disease. For the prevention of fungal infections in immunocompromised patients considered at risk as a consequence of neutropenia following cytotoxic chemotherapy or radiotherapy, the dose should be 3 mg/kg to 12 mg/kg once daily, depending on the extent and duration of the induced neutropenia (see Use in Adults). (For children with impaired renal function, see Use in Renal Impairment.). Use in Children 4 Weeks of Age and Younger Neonates excrete fluconazole slowly. In the first two weeks of life, the same mg/kg dosing as in older children should be used but administered every 72 hours. During Weeks 3 and 4 of life, the same dose should be given every 48 hours. Use in Elderly Where there is no evidence of renal impairment, normal dosage recommendations should be adopted. For patients with renal impairment (creatinine clearance <50 ml/min), the dosage schedule should be adjusted as described below. Use in Renal Impairment Fluconazole is predominantly excreted in the urine as unchanged drug. No adjustments in single-dose therapy are necessary. In patients (including children) with impaired renal function who will receive multiple doses of fluconazole, an initial loading dose of 50 mg to 400 mg should be given. After the loading dose, the daily dose (according to indication) should be administered as outlined in Table 1: 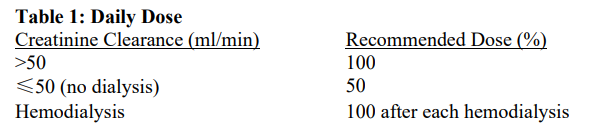 Patients on hemodialysis should receive 100% of the recommended dose after each hemodialysis; on non-dialysis days, patients should receive a reduced dose according to their creatinine clearance. Administration Fluconazole may be administered either orally (Capsules and Powder for Oral Suspension) or by intravenous infusion (Solution for Infusion) at a rate not exceeding 10 ml/min, the route being dependent on the clinical state of the patient. On transferring from the intravenous to the oral route, or _vice versa,_ there is no need to change the daily dosage. Fluconazole is formulated in 0.9% sodium chloride solution, each 200 mg (100 ml bottle) containing 15 mmol each of Na+ and Cl-. Because fluconazole is available as a dilute saline solution, in patients requiring sodium or fluid restriction, consideration should be given to the rate of fluid administration.
ORAL
Medical Information
**4.1 Therapeutic indications** Therapy may be instituted before the results of the cultures and other laboratory studies are known; however, once these results become available, anti-infective therapy should be adjusted accordingly. 1. Cryptococcosis, including cryptococcal meningitis and infections of other sites (e.g., pulmonary, cutaneous). Normal hosts and patients with AIDS, organ transplants or other causes of immunosuppression may be treated. Fluconazole can be used as maintenance therapy to prevent relapse of cryptococcal disease in patients with AIDS. 2. Systemic candidiasis, including candidemia, disseminated candidiasis and other forms of invasive candidal infections. These include infections of the peritoneum, endocardium, eye, and pulmonary and urinary tracts. Patients with malignancy, in intensive care units, receiving cytotoxic or immunosuppressive therapy, or with other factors predisposing to candidal infection may be treated. 3. Mucosal candidiasis. These include oropharyngeal, esophageal, non-invasive bronchopulmonary infections, candiduria, mucocutaneous and chronic oral atrophic candidiasis (denture sore mouth). Normal hosts and patients with compromised immune function may be treated. 4. Genital candidiasis. Vaginal candidiasis, acute or recurrent. 5. Prevention of fungal infections in patients with malignancy who are predisposed to such infections as a result of cytotoxic chemotherapy or radiotherapy. 6. Dermatomycosis, including tinea pedis, tinea corporis, tinea cruris, and dermal _Candida_ infections.
**4.3 Contraindications** Fluconazole should not be used in patients with known sensitivity to the drug, any of the inert ingredients or to related azole compounds. Co-administration of terfenadine is contraindicated in patients receiving fluconazole at multiple doses of 400 mg/day or higher based upon results of a multiple-dose interaction study. Co-administration of other drugs known to prolong the QT interval and which are metabolized via the enzyme CYP3A4 such as cisapride, astemizole, erythromycin, pimozide and quinidine are contraindicated in patients receiving fluconazole (see sections 4.4 **Special warnings and precautions for use** and 4.5 **Interaction with other medicinal products and other forms of interaction** – _please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information_).
J02AC01
fluconazole
Manufacturer Information
PFIZER PRIVATE LIMITED
PFIZER AUSTRALIA PTY LTD
Fareva Amboise
Active Ingredients
Documents
Package Inserts
Diflucan PI.pdf
Approved: September 15, 2022